Thursday, December 30, 2004
Rearranging the Deck Chairs...
I made some adjustments to the sidebar yesterday:
Yes, that's my mug over there, taken when I was a chief resident.
I have grouped some of my serial posts together as well:
Grand Rounds: links to the weekly summary of medical posts.
The Future of Surgery: a collection of posts relating to the evolving nature of surgical practice and training.
Practice Makes Perfect: posts about evidence-based medicine and surgery, especially studies comparing volume to outcome.
Tales from the Trauma Service/Operating Room: stories about patients that roll my way. These are the posts with the radiographs and intraoperative photographs. May not be suitable for all viewers.
Have a happy New Year's Day....I'm on call all weekend. |
I made some adjustments to the sidebar yesterday:
Yes, that's my mug over there, taken when I was a chief resident.
I have grouped some of my serial posts together as well:
Grand Rounds: links to the weekly summary of medical posts.
The Future of Surgery: a collection of posts relating to the evolving nature of surgical practice and training.
Practice Makes Perfect: posts about evidence-based medicine and surgery, especially studies comparing volume to outcome.
Tales from the Trauma Service/Operating Room: stories about patients that roll my way. These are the posts with the radiographs and intraoperative photographs. May not be suitable for all viewers.
Have a happy New Year's Day....I'm on call all weekend. |
This Job Could Really be Fun...
If some patients weren't such a pain. My latest example. I performed an aspiration of a breast cyst last week. It had the appearance of normal cyst fluid, but the patient was insistent about it being sent off for cytology. I asked the patient to return in a week to discuss the results.
When the day of the appointment came, the patient refused to pay the co-pay required by her insurance company. She then called several times demanding we give her the results over the telephone. She was told by my staff that it was my policy not to give biopsy results over the telephone. She asked that we fax the results to her referring physician's office. We did that but the physician in question declined to give her the results.
The next day she began calling again. She became increasingly rude to my staff and even threw the threat of litigation around. She demanded her records and they were provided for her. The cost of copying the records was slightly less than her co-pay. I sent her a dismissal letter today.
Now before I am accused of being a money-grubbing heartless bastard, let me get a few things out:
I don't give results out over the phone because I don't think it's right to tell someone they have cancer over the telephone. Why not just give negative results over the phone? Firstly it's not fair to those with cancer that they are kept in suspense and secondly the discussion of results gets the patient back into the office for a wound check. Oftentimes follow-up mammograms need to be ordered and if the patients get what they want (the biopsy report) they will often "skip out" on the follow-up appointment. I'm sure that my primary care colleagues have similar problems with discussion of lab results.
The procedure done on this patient had no global period, and my practice is required by the managed care contract to collect the co-pay. Even if we don't the patient will get the bill for the co-pay from their insurance carrier.
Sometimes it's not worth the trouble... |
If some patients weren't such a pain. My latest example. I performed an aspiration of a breast cyst last week. It had the appearance of normal cyst fluid, but the patient was insistent about it being sent off for cytology. I asked the patient to return in a week to discuss the results.
When the day of the appointment came, the patient refused to pay the co-pay required by her insurance company. She then called several times demanding we give her the results over the telephone. She was told by my staff that it was my policy not to give biopsy results over the telephone. She asked that we fax the results to her referring physician's office. We did that but the physician in question declined to give her the results.
The next day she began calling again. She became increasingly rude to my staff and even threw the threat of litigation around. She demanded her records and they were provided for her. The cost of copying the records was slightly less than her co-pay. I sent her a dismissal letter today.
Now before I am accused of being a money-grubbing heartless bastard, let me get a few things out:
I don't give results out over the phone because I don't think it's right to tell someone they have cancer over the telephone. Why not just give negative results over the phone? Firstly it's not fair to those with cancer that they are kept in suspense and secondly the discussion of results gets the patient back into the office for a wound check. Oftentimes follow-up mammograms need to be ordered and if the patients get what they want (the biopsy report) they will often "skip out" on the follow-up appointment. I'm sure that my primary care colleagues have similar problems with discussion of lab results.
The procedure done on this patient had no global period, and my practice is required by the managed care contract to collect the co-pay. Even if we don't the patient will get the bill for the co-pay from their insurance carrier.
Sometimes it's not worth the trouble... |
Wednesday, December 29, 2004
Why I Do what I Do....
A reader emails:
While it may seem cheesy, I have always wanted to be a physician. Even when I was younger I was really in to it. My grandparents gave me a paperback copy of Gray's Anatomy when I was nine or ten years old. This was fairly constant throughout high school until my junior year when I, for reasons I cannot recall, wanted to become an architect or civil engineer. I was even accepted in the College of Architecture at Georgia Tech. Then my girlfriend (now my wife) was in the hospital during my senior year for a prolonged illness. She recovered and I then changed my mind, my major, and my college. I worked in the emergency department of my local hospital during college and shadowed physicians during vacations. I was exposed to the community practice of cardiology, family practice, emergency medicine, internal medicine, pulmonology, orthopedic surgery, general surgery, and pediatrics. This gave me tremendous insight about medicine as a career. I had few illusions about what the "workaday life" of a physician was all about.
So after acceptance to medical school I was bouncing between cardiology and orthopedics. I wanted a specialty that would allow me to make a direct and immediate impact on patients and would allow me to care for patients of various ages and conditions. General surgery was somewhat a secondary concern until I started my third-year clinical rotations. I started with neurosurgery, perhaps the hardest rotation for students at the Medical College of Georgia. During that rotation I was taken under the wing of an intern who allowed me to place lines, taught me about TPN, and was the major force in getting me into general surgery. My fourth year was spent doing subinternships and away rotations in surgery.
My take on the future of surgical training is that the residency programs will have to extend the length of clinical training to six years due to the limitations placed on the programs by the 80-hour workweek. The residents probably aren't going to be able to get the case numbers they need.
As far as surgical practice, specialization will increase, this will be brought on by the increased popularity of fellowships, even though seventy percent already do. This will lead to what would be thought of as mutually exclusive events: surgeons becoming more specialized and more generalized. In the major metropolitan areas surgical care will become more specialist delivered while in rural areas more subspecialst care (especially endoscopy) will be delivered by general surgeons.
There will be a new subspecialist, the "emergency surgeon". This is already evolving from trauma/critical care surgeons in academic centers who are expanding their practice, and liking it. From the January 2004 Journal of Trauma:Trauma and Emergency Surgery: An Evolutionary Direction for Trauma Surgeons
So the community general surgeon will gradually fade away, due to diffusion of surgical subspecialists out of the large cities, and general surgeons who "self-specialize" in their own practices.
This site "So You Want to be a Surgeon" from the ACS is something that interested students may find helpful |
A reader emails:
I've always held career aspirations in the life sciences, but made sure to test these against other possibilities while in college. The end result: I still wanted to be a doctor, despite how much I've been told I'd be better off in research and won't have a life for the next 7-9 years. While I was volunteering in an emergency room, I had the fortune of working with some great ER docs who let me watch everything they did and loved explaining every step of the way. As a result of my hours in the ER and mechanical inclinations (I was always a fan of pulling stuff apart when I was growing up to see the guts and machinations of everything from TVs and radios to grandfather clocks) I am seriously considering surgery as a career choice. I couldn't tell you a subspecialty yet, but I've entertained the ideas of orthopedics, plastics, craniofacial, cardiothoracic, and neuro (though like many I'm sure, I have an inherent doubt in my ability to work in such a mentally demanding and complex field, not to mention the $383,000 insurance premiums!).
So I wanted to get your story on surgery: how you 'fell in love' with it, the pros/cons, if you were one of the ones who knew before matriculation or if you decided late in schooling, how this career choice affected your choice in clinical rotations, what your views on the future of surgery are, etcetera.
While it may seem cheesy, I have always wanted to be a physician. Even when I was younger I was really in to it. My grandparents gave me a paperback copy of Gray's Anatomy when I was nine or ten years old. This was fairly constant throughout high school until my junior year when I, for reasons I cannot recall, wanted to become an architect or civil engineer. I was even accepted in the College of Architecture at Georgia Tech. Then my girlfriend (now my wife) was in the hospital during my senior year for a prolonged illness. She recovered and I then changed my mind, my major, and my college. I worked in the emergency department of my local hospital during college and shadowed physicians during vacations. I was exposed to the community practice of cardiology, family practice, emergency medicine, internal medicine, pulmonology, orthopedic surgery, general surgery, and pediatrics. This gave me tremendous insight about medicine as a career. I had few illusions about what the "workaday life" of a physician was all about.
So after acceptance to medical school I was bouncing between cardiology and orthopedics. I wanted a specialty that would allow me to make a direct and immediate impact on patients and would allow me to care for patients of various ages and conditions. General surgery was somewhat a secondary concern until I started my third-year clinical rotations. I started with neurosurgery, perhaps the hardest rotation for students at the Medical College of Georgia. During that rotation I was taken under the wing of an intern who allowed me to place lines, taught me about TPN, and was the major force in getting me into general surgery. My fourth year was spent doing subinternships and away rotations in surgery.
My take on the future of surgical training is that the residency programs will have to extend the length of clinical training to six years due to the limitations placed on the programs by the 80-hour workweek. The residents probably aren't going to be able to get the case numbers they need.
As far as surgical practice, specialization will increase, this will be brought on by the increased popularity of fellowships, even though seventy percent already do. This will lead to what would be thought of as mutually exclusive events: surgeons becoming more specialized and more generalized. In the major metropolitan areas surgical care will become more specialist delivered while in rural areas more subspecialst care (especially endoscopy) will be delivered by general surgeons.
There will be a new subspecialist, the "emergency surgeon". This is already evolving from trauma/critical care surgeons in academic centers who are expanding their practice, and liking it. From the January 2004 Journal of Trauma:Trauma and Emergency Surgery: An Evolutionary Direction for Trauma Surgeons
Background : The success of nonoperative management of injuries has diminished the operative experience of trauma surgeons. To enhance operative experience, our trauma surgeons began caring for all general surgery emergencies. Our objective was to characterize and compare the experience of our trauma surgeons with that of our general surgeons.
Methods : We reviewed records to determine case diversity, complexity, time of operation, need for intensive care unit care, and payor mix for patients treated by the trauma and emergency surgery (TES) surgeons and elective practice general surgery (ELEC) surgeons over a 1-year period.
Results : TES and ELEC surgeons performed 253 +/- 83 and 234 +/- 40 operations per surgeon, respectively (p = 0.59). TES surgeons admitted more patients and performed more after-hours operations than their ELEC colleagues. Both groups had a mix of cases that was diverse and complex.
Conclusion : Combining the care of patients with trauma and general surgery emergencies resulted in a breadth and scope of practice for TES surgeons that compared well with that of ELEC surgeons.
So the community general surgeon will gradually fade away, due to diffusion of surgical subspecialists out of the large cities, and general surgeons who "self-specialize" in their own practices.
This site "So You Want to be a Surgeon" from the ACS is something that interested students may find helpful |
Tuesday, December 28, 2004
What Have You Done for me Lately???
From the never look a gift horse in the mouth department and The Washington Times: U.N. official slams U.S. as 'stingy' over aid
But even the stingy U.S. is more charitable than other countries:
Americans and their government are the most charitable in the world, yet obviously this is not enough for some. Again from The Washington Times
From the never look a gift horse in the mouth department and The Washington Times: U.N. official slams U.S. as 'stingy' over aid
The Bush administration yesterday pledged $15 million to Asian nations hit by a tsunami that has killed more than 22,500 people, although the United Nations' humanitarian-aid chief called the donation "stingy."
"The United States, at the president's direction, will be a leading partner in one of the most significant relief, rescue and recovery challenges that the world has ever known," said White House deputy press secretary Trent Duffy.
But U.N. Undersecretary-General for Humanitarian Affairs Jan Egeland suggested that the United States and other Western nations were being "stingy" with relief funds, saying there would be more available if taxes were raised.
But even the stingy U.S. is more charitable than other countries:
Offers of aid have poured in from around the world in the past two days, with the European Union's executive arm releasing $4 million in emergency aid and pledging an additional $27 million. Canada and several European nations — including Spain, Germany, Ireland and Belgium — each pledged about $1 million yesterday.And Secretary of State Colin Powell says more is on the way:
Secretary of State Colin L. Powell hinted that the $15 million U.S. offer was only the first installment of a larger aid package to those countries devastated by 30-foot waves triggered by a massive underwater earthquake.
"We also have to see this not just as a one-time thing," he said. "Some 20-plus thousand lives have been lost in a few moments, but the lingering effects will be there for years.
"The damage that was caused, the rebuilding of schools and other facilities will take time," he added. "So you need a quick infusion to stabilize the situation, take care of those who have been injured, get immediate relief supplies in, and then you begin planning for the longer haul."
Americans and their government are the most charitable in the world, yet obviously this is not enough for some. Again from The Washington Times
The same reliance on private forces and individual initiative is evident in American patterns of giving, which also deviate markedly from the rest of the world.If you wish to participate in that "extraordinary" giving for the tsunami victims here is a good place to start. I'm sure those organizations won't complain about your contribution being "stingy". With billions of dollars wasted by the UN Oil-for-Food program, the UN is no position to tell others how to spend their money. The gall of some people. |
The U.S. government ranked 22nd among the world's developed nations in 2003 in foreign aid on a per-capita basis, according to the Organization for Economic Cooperation and Development, offering one-sixth the amount of aid per citizen offered by Norway.
But private philanthropy in America is one of the most powerful and effective aid programs on earth, concludes a new study by researchers at the Institute for Jewish and Community Research.
American private charities are set to spend more than $200 billion this year, and more than half of U.S. adults will work on volunteer projects, putting in an estimated 20 billion hours in donated time.
One study by the Washington-based Philanthropy Roundtable found that the average American household contributes seven times as much to charity as its German counterpart, and Americans are six times more likely than Germans to do volunteer work.
"In short," researchers Alexander Karp, Gary A. Tobin and Aryeh Weinberg write in the journal Philanthropy, "American philanthropy is extraordinary by any world standard and the reason is that America herself is exceptional."
Monday, December 27, 2004
Tales From the Trauma Service III.....
Another case picked up by my partner.
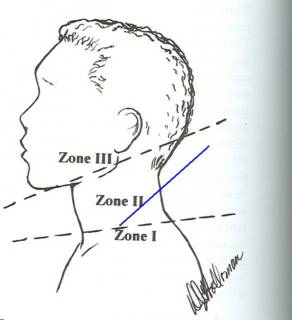
20-ish year old stabbed in the left neck in zone I. For your information here are the anatomical division of the neck described by Monson in 1969:
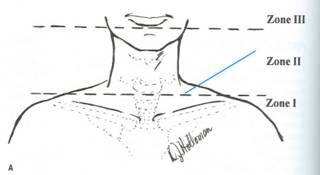
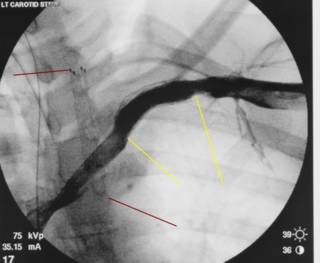
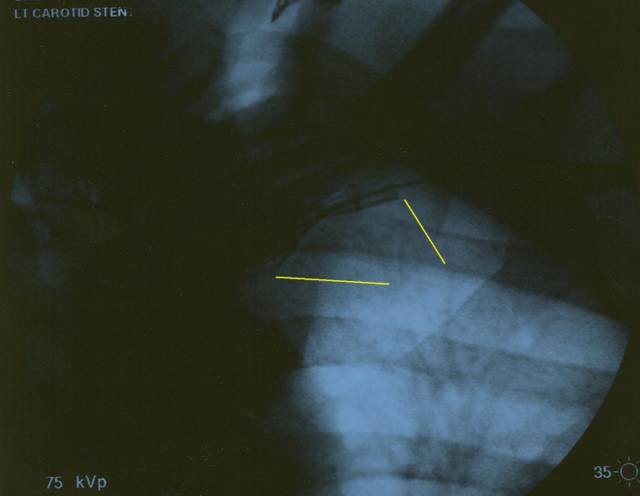
The blue lines indicate the location of the wound. There was active bleeding and a bruit and thrill over the neck so the patient was taken to angiogram which revealed a common carotid to jugular fistula. (images poor). The neck was explored and packed as no stent-graft was readily available. One became available the next day:
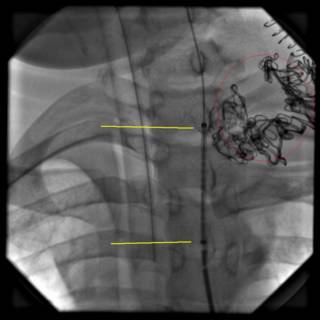
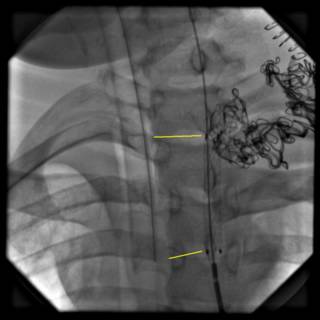
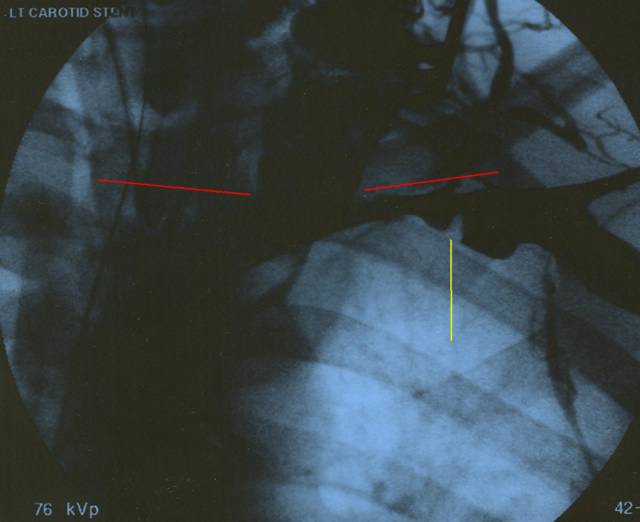
The black squiggly lines in the upper right are from packing left in place from the exploration. Attempts were made to remove the packing yet again, but bleeding continued. The patient was then taken to the OR again for possible sternotomy for repair of what was thought to be the inominate vein. Another attempt would be made for an endovascular repair. The patient was found to have thrombosed his internal jugular vein on that side with a thrombosis in his axillary vein as well. The axillary DVT was thrombolysed with an Angiojet. The following images are from the endovascular repair. I apologize in advance for the quality:
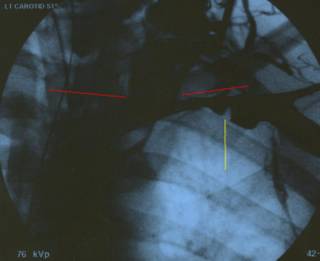
The yellow line represents the subclavian vein, the green lines represent the extravasated contrast in the injured area.
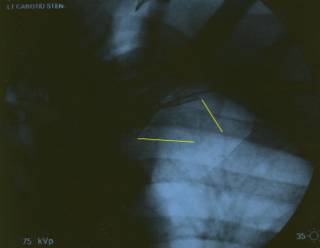
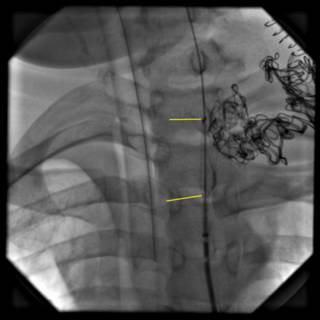
The yellow lines indicate the stent in situ. Importantly there is no further leak of contrast.
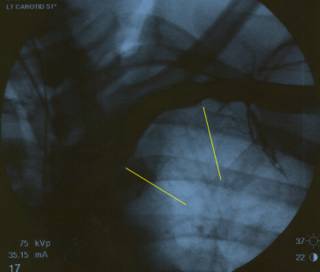
Good flow through the stent. Here is a better image:
He was extubated on postop day 3, and is progressing.
Another case picked up by my partner.
20-ish year old stabbed in the left neck in zone I. For your information here are the anatomical division of the neck described by Monson in 1969:
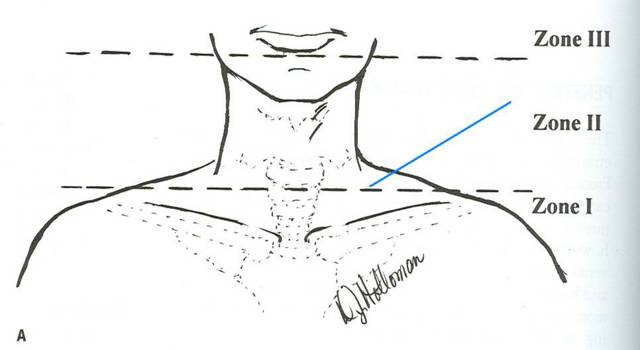
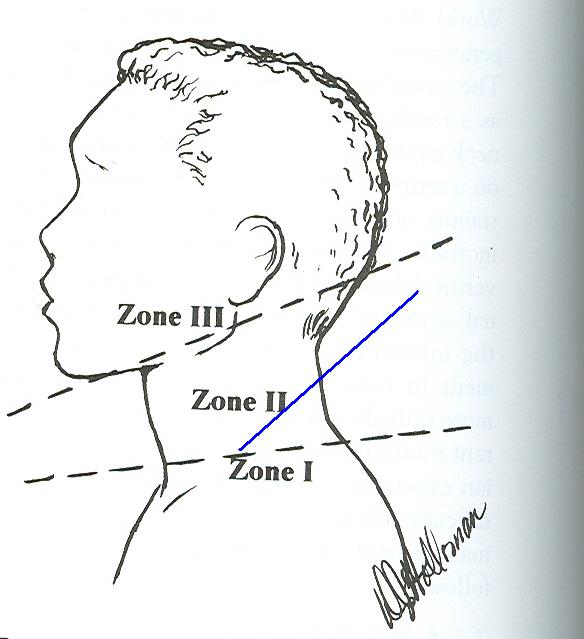
The blue lines indicate the location of the wound. There was active bleeding and a bruit and thrill over the neck so the patient was taken to angiogram which revealed a common carotid to jugular fistula. (images poor). The neck was explored and packed as no stent-graft was readily available. One became available the next day:



The black squiggly lines in the upper right are from packing left in place from the exploration. Attempts were made to remove the packing yet again, but bleeding continued. The patient was then taken to the OR again for possible sternotomy for repair of what was thought to be the inominate vein. Another attempt would be made for an endovascular repair. The patient was found to have thrombosed his internal jugular vein on that side with a thrombosis in his axillary vein as well. The axillary DVT was thrombolysed with an Angiojet. The following images are from the endovascular repair. I apologize in advance for the quality:
The yellow line represents the subclavian vein, the green lines represent the extravasated contrast in the injured area.
The yellow lines indicate the stent in situ. Importantly there is no further leak of contrast.

Good flow through the stent. Here is a better image:

He was extubated on postop day 3, and is progressing.
Labels: Tales from the Trauma Service
|Friday, December 24, 2004
Merry Christmas....

From the second chapter of the Gospel of Luke:
Best wishes for you and your family this holiday. I'll be back on Monday.
|

From the second chapter of the Gospel of Luke:
And it came to pass in those days, that there went out a decree from Caesar Augustus, that all the world should be taxed. (And this taxing was first made when Cyrenius was governor of Syria.)
And all went to be taxed, every one into his own city. And Joseph also went up from Galilee, out of the city of Nazareth, into Judea, unto the city of David, which is called Bethlehem (because he was of the house and lineage of David), to be taxed with Mary his espoused wife, being with child.
And so it was, that, while they were there, the days were accomplished that she should be delivered. And she brought forth her firstborn son, and wrapped him in swaddling clothes, and laid him in a manger; because there was no room for them in the inn.
And there were in the same country shepherds abiding in the field, keeping watch over their flock by night. And lo, the angel of the Lord come upon them, and the glory of the Lord shone round about them: and they were sore afraid.
And the angel said unto them, "Fear not: for, behold, I bring you good tidings of great joy, which shall be to all people. For unto you is born this day in the city of David a Savior, which is Christ the Lord. And this shall be a sign unto you; Ye shall find the babe wrapped in swaddling clothes, lying in a manger."
And suddenly there was with the angel a multitude of the heavenly host praising God, and saying, "Glory to God in the highest, and on earth peace, good will toward men."
Best wishes for you and your family this holiday. I'll be back on Monday.
|
Fun with Interventional Radiology....
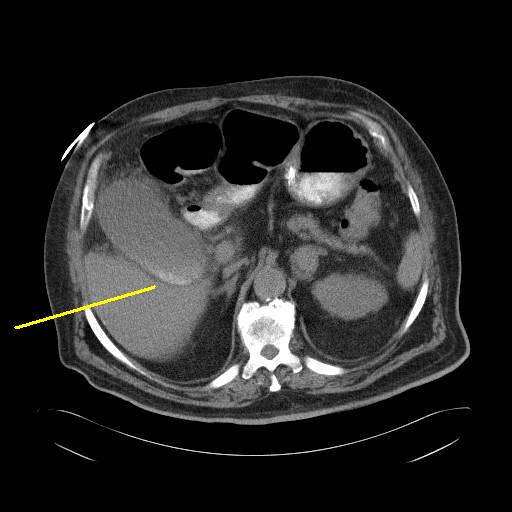
Asked to see a 70-ish man admitted with altered mental status. History of severe COPD and diabetes. Develops an acute MI. Found to have abdominal pain and gallbladder sludge. WBC's 20,000 and patient becomes hypotensive. CT scan obtained:

Some ascities.

Stones within a hydropic gallbladder.
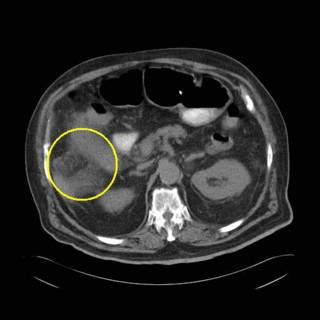
inflammatory changes in the right upper quadrant.
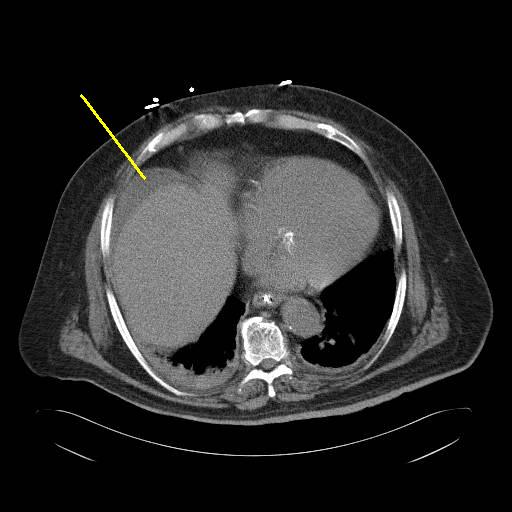
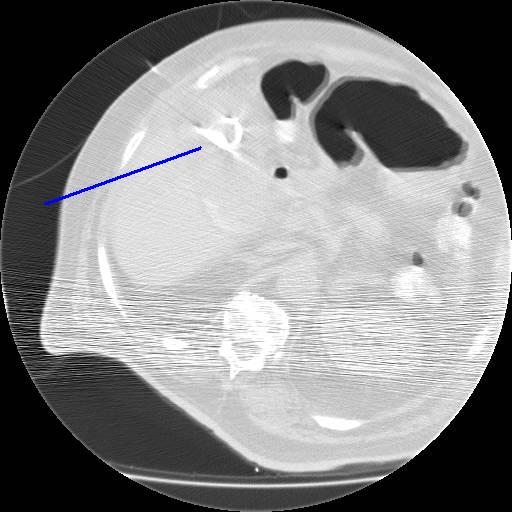
The last thing this patient needs is an operation, fortunately there is another option, a cholecystostomy tube. It will allow the gallbladder to be decompressed and may be left in place indefinitely. The patient can undergo cholecystectomy when medically stable.

The needle inserted percutaneously.

One cut of the 8 french pigtail.
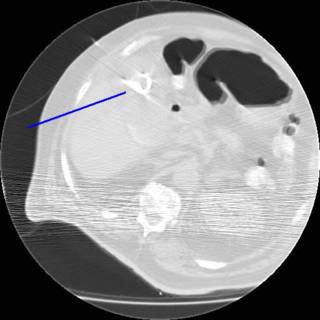
The pigtail within the gallbladder.
Afebrile today with WBC down to 13,000. BP and mental status improved. |
Asked to see a 70-ish man admitted with altered mental status. History of severe COPD and diabetes. Develops an acute MI. Found to have abdominal pain and gallbladder sludge. WBC's 20,000 and patient becomes hypotensive. CT scan obtained:
Some ascities.
Stones within a hydropic gallbladder.

inflammatory changes in the right upper quadrant.
The last thing this patient needs is an operation, fortunately there is another option, a cholecystostomy tube. It will allow the gallbladder to be decompressed and may be left in place indefinitely. The patient can undergo cholecystectomy when medically stable.

The needle inserted percutaneously.

One cut of the 8 french pigtail.
The pigtail within the gallbladder.
Afebrile today with WBC down to 13,000. BP and mental status improved. |
Thursday, December 23, 2004
The Future of Surgery VII....
From the November edition of the Journal of the American College of Surgeons:General surgery as a career: A contemporary review of factors central to medical student specialty choice
There is much of the usual "lifestyle issue" that works against general surgery, of course, but it seems that medical students are a wishy-washy lot:
So more medical students fall out of love with surgery than fall in love with it. My colleagues in academia often times do not provide a positive "role model" for students:
So while the FP faculty does an excellent job in fostering interest among the preclinical students, the surgical faculty does poorly, allowing the "badmouthing" that 91% of prospective surgeons hear about their calling.
So what to do? The authors suggest an increased mentoring presence by the faculty for the first and second year. Will this "selling of surgery" help offset the "lifestyle issue"? Time will tell
From the November edition of the Journal of the American College of Surgeons:General surgery as a career: A contemporary review of factors central to medical student specialty choice
There is much of the usual "lifestyle issue" that works against general surgery, of course, but it seems that medical students are a wishy-washy lot:
It appears that 14% of medical students have made their specialty choice before entering medical school, and an additional 41% to 45% of students make their specialty choice before their third year of medical school, before having had any clinical experiences. It is notable that general surgery is among the most popular specialties among medical students at matriculation.
Though many medical students make early decisions on choice of specialties, these decisions often change. Only 20% to 45% of medical students ultimately choose the specialty that they initially would have preferred if asked to choose before their first medical school lecture. About half of the students who ultimately match in their initial preference had changed their decision at some point before returning to their original choice. The other half never wavered from their original choice. Career choice remains at least as stable as students progress through medical school, reaching 69% in some studies. These numbers are similar for surgery in particular, with 40% to 60% of students initially interested in surgery changing their minds to pursue other specialties at some time during medical school. That being said, a medical student's choice of surgery as a career appears slightly more stable than the choice of most other specialties. Interestingly, it has been noted that premedical, summer, or extracurricular clinical experiences increase the certainty of choice, regardless of chosen specialty.
Many medical students, as noted in the preceding text, initially interested in general surgery eventually lose this interest and instead favor another career choice at some point during medical school. Though some medical students not initially interested in surgery do become interested at some point between matriculation and graduation, these are outnumbered by those initially interested in surgery who eventually choose other careers. The number of students who match into general surgery programs, as a result, is much smaller than the number of medical students initially interested in the specialty. In other words, there is a net efflux of interested medical students from general surgery to other specialties. In comparison, few medical students are interested in anesthesiology at matriculation, but many become interested in the specialty at some point during medical school, resulting in a net influx. Though many medical students initially interested in family practice change their decision, this number is offset by students who become interested in family practice. The result is a net balance.
So more medical students fall out of love with surgery than fall in love with it. My colleagues in academia often times do not provide a positive "role model" for students:
About 50% of medical students, as noted above, who choose surgery as a career and do not change their minds make this choice by the end of their second year of school, before any clinical experiences in surgery. Yet few efforts are made to mentor preclinical medical students in most medical schools, despite the fact that this may increase interest in general surgery.
Perhaps because of the absence of surgeons in preclinical undergraduate medical education, communication between medical students comprised more than 80% of the information second year students get about surgery, according to one study. It appears that students may have some influence on the career choices of one another through the negative comments, or "badmouthing" as described by some authors, of particular specialties. Indeed, one survey of 1,114 medical students reported that 76% of medical students heard negative comments about their career choice, sometimes as early as their first or second year of medical school. Surgery was the specialty most frequently criticized; 91% of students with interest in surgery reported hearing negative comments about the specialty. In contrast, pediatrics was the least frequently criticized; only 57% of students interested in pediatrics reported hearing negative comments. Seventeen percent of all respondents reported altering their career choice in response to these negative comments.
The importance of mentors or role models cannot be overstated. Medical students encouraged by role models to pursue a surgical career are less likely to be discouraged by lifestyle, time commitment, call schedules, or length of residency. Mentors may be especially influential when the personalities of the student and mentor are agreeable. Many students become interested in or choose surgery as a specialty after a rotation and exposure to mentors in that field. Seventy-three percent of medical students undecided on specialty choice and 80% of students who change their choice of specialty during the third year of clerkship eventually choose specialties they had experienced during the first half of the third year. Seventy-nine percent of students were influenced "very much" or "some" by faculty members during their surgery clerkship.
Although surgery faculty typically serve as role models or mentors for surgery students, residents also play a vital role in teaching and mentoring medical students. In one survey of 123 medical students, residents were notably more active in 14 of 15 teaching behaviors surveyed. The surveyed behaviors included physical diagnosis and bedside procedures and stimulating students to do additional reading, teaching students to be more analytical, and serving as role models. Residents were also rated as having a positive influence on the students' attitudes toward general surgery (p = 0.007). Indeed, resident teaching was viewed as more important than attending physician teaching, nurses' teaching, seminars, operating room experience, clinic experience, and conferences. Only independent reading and tutorials were viewed as more important.
The influence of role models or mentors may have either a very positive or a very negative impact on medical students' perceptions of the field of surgery. Students often make note of not only individual characteristics, but also how role models interact with patients, residents, and other physicians. The negative impact a poor role model may have was illustrated during a focus group discussion with one medical student:
[S]urgeons, I have to say honestly, they shred each other to pieces. That was a huge turn-off. I can stand sleep deprivation for ten years, but I can't stand five minutes with the way they get at each other; to be rude to each other, to be rude to the house officers who couldn't fight back, and to be rude to the students who couldn't say anything in defense.
Student perceptions of surgeons and surgical careers may be influenced by their third-year surgery clerkship. One questionnaire-based study reported that both students' ratings of surgeon compassion and respect for surgeons increased during the clerkship, though ratings of surgeon collegiality with other physicians and surgeon commitment to teaching decreased. There was no net interest in surgical careers during the clerkship.
Finally, operative experiences during a medical student's clerkship may affect interest in surgery. Students pursuing careers in most surgical subspecialties (including cardiothoracic, transplant, plastics, and pediatric surgery) have observed substantially more procedures in their chosen subspecialty field than have other students. In a similar study, exposure to general surgical procedures during the third year clerkship correlated to interest in general surgery, and no such correlation existed between exposure to general surgical procedures or surgical subspecialty procedures and interest in surgical subspecialties. It is not clear whether these experiences help determine interest in these surgical subspecialties or if such experiences were sought because of certain interests.
So while the FP faculty does an excellent job in fostering interest among the preclinical students, the surgical faculty does poorly, allowing the "badmouthing" that 91% of prospective surgeons hear about their calling.
So what to do? The authors suggest an increased mentoring presence by the faculty for the first and second year. Will this "selling of surgery" help offset the "lifestyle issue"? Time will tell
Labels: Future of Surgery
|
How Far We Have Come...
New York Times article on the golden anniversary today of the first successful solid organ transplant:The Ultimate Gift: 50 Years of Organ Transplants
An effort for which Dr. Murray won a Nobel Prize.
From Dr. Starzl:
What will the next fifty years hold?
New York Times article on the golden anniversary today of the first successful solid organ transplant:The Ultimate Gift: 50 Years of Organ Transplants
The first successful organ transplant recipient was a 23-year-old man from Northboro, Mass., named Richard Herrick, who had just been discharged from the Coast Guard.
On Dec. 23, 1954, he received a kidney from his healthy identical twin brother, Ronald, in an operation performed by Dr. Joseph E. Murray at what is now Brigham and Women's Hospital in Boston. Richard survived for eight years until the original kidney disease destroyed his new organ.
Mr. Herrick's surgery was a victory long in coming. The very first transplants were blood transfusions, procedures that became much safer after the discovery of blood groups in 1900. In 1905, doctors performed the first corneal transplant, and then moved on to solid organs.
But for many years, they had no real success. Beginning with the first attempted transplant of a human kidney in France in 1906, doctors performed about 40 kidney transplants, but all the patients died. In some early transplants, the donor kidney was placed not in the pelvis, as is now standard practice, but in areas like the arm or thigh.
In June 1950, a Chicago surgeon removed one of a woman's two failing cystic kidneys and gave her a healthy organ that functioned for at least 53 days. But the organ was rejected sometime in the next months.
Still, the woman lived five more years, probably because the donor organ survived long enough to allow her damaged kidney to recover partial function, Dr. Nicholas L. Tilney, also of Brigham and Women's, wrote in "Transplant: From Myth to Reality." But Mr. Herrick's is considered the first successful transplant because experts defined success as survival of a graft for at least a year.
In their struggle to make transplants work, the pioneers had to overcome the objections of antivivisectionists to conduct the animal experiments needed to develop the techniques for human transplants. They also knew that a failed operation could set the field back by decades, Dr. Murray said.
The radical nature of an operation to remove a healthy organ from a donor led Dr. Murray's team to seek support from religious, legal and community leaders. Nevertheless, critics accused the doctors of playing God. Dr. Starzl recalled how participants at scientific meetings lampooned his and other surgeons' first - and often disappointing - reports.
An effort for which Dr. Murray won a Nobel Prize.
From Dr. Starzl:
"The growth of transplantation from ground zero to its present state seems like a fairy tale, a fantasy that became reality because of the courage of our patients," said Dr. Thomas E. Starzl, a pioneering transplant surgeon who led the team that performed Mr. Phillips's operation and now is at the University of Pittsburgh. "The truth is that none of us in the 1950's remotely envisioned the height to which transplantation would rise and the way it has changed the face of medicine. Transplants have had trickle down effects on all aspects of society like acceptance of criteria for brain death, passage of anatomical gift acts and the growth of biomedical ethics."
What will the next fifty years hold?
Labels: Transplantation
|Wednesday, December 22, 2004
Don't Let Me Touch Your Breasts....
As they likely will have cancer. Three women over the past five weeks:
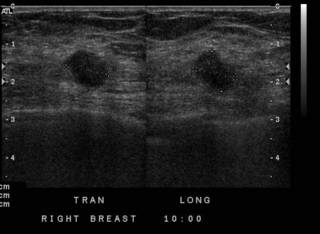
70-ish female with a several year history of breast mass, but was "afraid" to have it evaluated. Only went to the doctor when it became painful and her nipple retracted. She was too tender to have a mammogram. In office ultrasound:
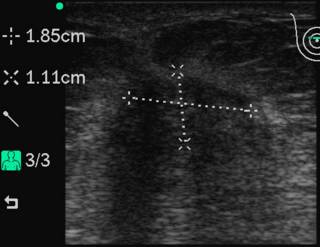
With a Sonosite 180, this is the transverse view. We then went to a core biopsy:
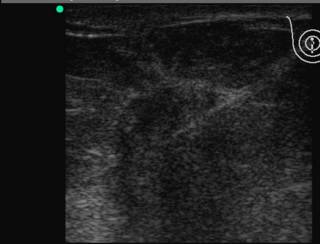
The white line is the needle. It was positive for invasive lobular cancer. She elected to have a mastectomy. She had the only enlarged level III nodes I have encountered in my career. 19 out of 20 nodes were positive. Ignorance is not always bliss.
40-ish with a newly-discovered mass. She was seen by another physician who sent her to the radiologist for a core biopsy:
The core biopsy revealed "stromal fibrosis". One of the disadvantages of core biopsy is the possibility of sample error. If the path report doesn't agree with the clinical scenario, don't trust it. She underwent an open wire-localized biopsy which revealed invasive cancer. She chose breast conservation. Her lumpectomy specimen had DCIS within it, not seen on earlier biopsies. Had I known this I may have tried to steer her toward mastectomy and reconstruction, given the increased chances of recurrence. The post-lumpectomy radiation will help take care of it.
Lastly a 60-ish woman with an abnormal mammogram, unfortunately her diagnostic films did not scan well, but her compression and localization films did:
Here is the ultrasound:
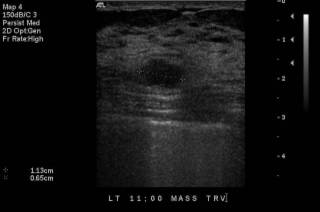

She opted for excisional biopsy. Yet again, a malignant diagnosis. She opted for a mastectomy, scheduled for the Monday after Christmas. |
As they likely will have cancer. Three women over the past five weeks:
70-ish female with a several year history of breast mass, but was "afraid" to have it evaluated. Only went to the doctor when it became painful and her nipple retracted. She was too tender to have a mammogram. In office ultrasound:
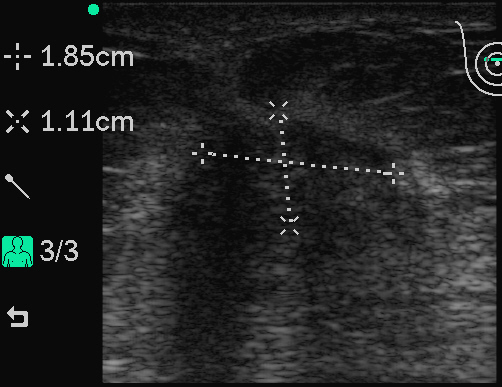
With a Sonosite 180, this is the transverse view. We then went to a core biopsy:
The white line is the needle. It was positive for invasive lobular cancer. She elected to have a mastectomy. She had the only enlarged level III nodes I have encountered in my career. 19 out of 20 nodes were positive. Ignorance is not always bliss.
40-ish with a newly-discovered mass. She was seen by another physician who sent her to the radiologist for a core biopsy:

The core biopsy revealed "stromal fibrosis". One of the disadvantages of core biopsy is the possibility of sample error. If the path report doesn't agree with the clinical scenario, don't trust it. She underwent an open wire-localized biopsy which revealed invasive cancer. She chose breast conservation. Her lumpectomy specimen had DCIS within it, not seen on earlier biopsies. Had I known this I may have tried to steer her toward mastectomy and reconstruction, given the increased chances of recurrence. The post-lumpectomy radiation will help take care of it.
Lastly a 60-ish woman with an abnormal mammogram, unfortunately her diagnostic films did not scan well, but her compression and localization films did:
Here is the ultrasound:


She opted for excisional biopsy. Yet again, a malignant diagnosis. She opted for a mastectomy, scheduled for the Monday after Christmas. |
Tuesday, December 21, 2004
Holiday Cheer...
I live in a neighborhood where Clark Griswold would struggle to keep up with the Jones' in the Christmas decorating. Our neighbor has all of their stuff on a timer, including one of those inflatable Santa Clauses. Santa usually looks like he is on a bender:

HO!!HO!!HO!! |
I live in a neighborhood where Clark Griswold would struggle to keep up with the Jones' in the Christmas decorating. Our neighbor has all of their stuff on a timer, including one of those inflatable Santa Clauses. Santa usually looks like he is on a bender:

HO!!HO!!HO!! |
Monday, December 20, 2004
The Trauma Tax...
From the Atlanta Business Chronicle: New driver fines may help state's 14 trauma centers
A "trauma fund" would be beneficial because the money could be used to induce more of the specialists such as orthopedists and neurosurgeons to participate in the trauma system. It could also induce more hospitals to participate, as wide areas of the state are uncovered. The full listing of the trauma centers is here. The geographical distribution is illustrated here:

The level I centers are red, the level II's are blue, level III's green and the sole level IV is gray. As you can see there are wide areas of the state that are uncovered, especially in the northeast, south, and southeast. Patients in these areas aren't turned away, but the care may not be as ideal as in a trauma center. While usually against new taxes, these strike me more as user's fees. |
From the Atlanta Business Chronicle: New driver fines may help state's 14 trauma centers
People who are caught driving unsafely would have to pay extra fees to help fund trauma centers if the CEO of Grady Health System gets his way.
In the face of rising medical costs and Medicaid cutbacks, Grady CEO Dr. Andy Agwunobi said he plans to ask the General Assembly to consider a new plan to help fund the state's 14 trauma centers. Agwunobi suggests Georgia adopt legislation that would fine people who are caught driving without seat belts or under the influence of drugs or alcohol, and use the money for a trauma center fund. He said the program has been used successfully in Texas. New Jersey also has a similar program.
"There is some harmony in the idea of -- instead of a fee charged to everybody -- having it charged to people who drive up the costs," Agwunobi said.
Trauma centers typically carry a heavy responsibility for caring for the uninsured, especially at Grady, where only 7 percent of patients have commercial insurance and many are covered by Medicaid. Agwunobi said proposed Medicaid cutbacks could hit the hospital hard overall, having a negative financial impact of $15 million to $39 million.
In Georgia, unreimbursed trauma care costs hospitals $200 million a year, and costs Grady alone at least $30 million a year, Agwunobi said. However, he said those costs often are invisible to the public.
"Unless you have a family member who gets in an accident, you don't think about it," Agwunobi said. "But we'll keep fighting for this; it's really about the 16-year-old boy who lives in Cordele, Ga., and gets in an accident and needs help."
Nationwide, as many as 35 percent of trauma patients who die do so because optimal care is not available, according to a 2004 study from the Centers for Disease Control and Prevention.
A "trauma fund" would be beneficial because the money could be used to induce more of the specialists such as orthopedists and neurosurgeons to participate in the trauma system. It could also induce more hospitals to participate, as wide areas of the state are uncovered. The full listing of the trauma centers is here. The geographical distribution is illustrated here:

The level I centers are red, the level II's are blue, level III's green and the sole level IV is gray. As you can see there are wide areas of the state that are uncovered, especially in the northeast, south, and southeast. Patients in these areas aren't turned away, but the care may not be as ideal as in a trauma center. While usually against new taxes, these strike me more as user's fees. |
Country Roads, Take Me (to the funeral) Home.....
No wonder I stay so busy:Country roads can be deadly
Based on this research from Georgia Tech. Some of the reasons given in the report:
They are examining the number of deaths, not of total crashes. The proposed theories have to do more with crash causation than deaths. Certainly if more crashes occur, more victims are expected to succumb to their injuries.
I think another reason could contribute, the lack of a well-developed trauma/EMS system in the rural southeast, especially in rural south Georgia. As seen in this article from the Atlanta Journal-Constitution I posted on in January, Georgia has a lot of work to do:
So are the deaths due to bad roads, or bad medical infrastructure? |
No wonder I stay so busy:Country roads can be deadly
The South's beautiful tree-lined roadways may be to blame for the region having the highest number of vehicle deaths in the country, according to a Georgia Institute of Technology study.
More than a quarter of U.S. vehicle deaths between 1996 and 2000 happened in just eight Southeast states - Georgia, South Carolina, North Carolina, Alabama, Mississippi, Kentucky, Florida and Tennessee. It's the largest proportion of deaths in any region of the country, according to the study.
The reason for the higher number of crashes is that the Southeast has a higher density of rural roads than any other part of the country. Driving on those roads has been dangerous for drivers. Sixty-four percent of the fatal crashes in the Southeast were on rural roads.
"The most frequent crashes in the Southeast occurred on rural roads in wooded areas where people ran off the road and hit a tree," said Karen Dixon, associate professor of civil and environmental engineering at Georgia Tech......
.....A lack of road maintenance funding in rural areas may mean country roads are loaded with driving hazards, such as trees that stand too close to the roadway, a lack of paved shoulders and devices such as rumble strips, Dixon said.
There were more than 49,000 fatal crashes in the Southeast out of nearly 186,600 fatalities on the road in the United States during the time period of the study.
Based on this research from Georgia Tech. Some of the reasons given in the report:
On rural roads, the most common contributing factor to traffic fatalities was late-night driving by tired or apparently intoxicated motorists, especially on weekends, Dixon noted. Many of these victims were males between ages 16 and 25.
The study also found that 48.6 percent of the regions fatal crashes involved drivers who did not wear seatbelts, she added. In a related finding in Georgias report, Dixon discovered a disproportionate number of pickup trucks involved in fatal crashes.....
Another of the studys findings lays potential blame for fatal crashes on the 2.5- to 5-inch pavement drop-offs often found on rural highway edges.
"Almost half of the non-state maintained roadway crashes we looked at had an edge drop-off issue, she noted. We dont know if this caused all of these crashes, but nonetheless, the potential exists for it to be a serious problem.
Drop-offs develop as roads are repaved and/or soil erodes along the shoulder. And roadside ruts are caused by rural mail carriers who drive with one side of their vehicles on the road and the other on the unpaved shoulder, she added.
They are examining the number of deaths, not of total crashes. The proposed theories have to do more with crash causation than deaths. Certainly if more crashes occur, more victims are expected to succumb to their injuries.
I think another reason could contribute, the lack of a well-developed trauma/EMS system in the rural southeast, especially in rural south Georgia. As seen in this article from the Atlanta Journal-Constitution I posted on in January, Georgia has a lot of work to do:
Lurking under Georgia's radar screen is a public health care crisis that costs hundreds of people their lives each year.
"If Georgia did nothing but become average, we'd save more than 600 lives a year," said Dr. James Patrick O'Neal, state Emergency Medical Services medical director. "If we had a statewide trauma network, we'd save more lives than that."
Vast chunks of Georgia remain unserved by a trauma center, hospitals qualified, equipped and staffed to treat people severely injured in car crashes or other mishaps. Only 14 of the state's hospitals meet the criteria to be designated as trauma centers, and only four, including Atlanta's Grady Memorial Hospital, are designated as Level 1, qualified to give the most extensive level of care.
South of Macon, there is only one Level 1 center, Savannah's Memorial Health University Medical Center.
A large group of Georgia lawmakers heard a heartfelt plea from health care professionals and safety advocates at a Thursday breakfast gathering to do more to address the lack of quality trauma care.
"It is costing more and more to provide this service," said Dr. M. Gage Ochsner, the Savannah facililty's director of trauma services. "Most of our trauma centers have provided it as a community service, but when it starts driving them into the ground, they have to look at [eliminating] it."
O'Neal said two-thirds of Georgia's hospitals are operating in the red, making it more difficult to justify providing expensive trauma coverage.
Complicating the issue even further, said Ken Beverly, chairman of the board for the Georgia Hospital Association, is Georgia's lack of a Good Samaritan law shielding physicians from many of the liabilities involved in emergency room work.
"Doctors don't want to go into emergency rooms," he said.
Injury is the leading cause of death for all Georgians aged 1 to 45, and ranks fourth among Georgians of all ages. It costs us 4,500 lives a year, hundreds of which could be saved if they could be reached, taken to a trauma center and treated within the famous "golden hour."
Yet many Georgians are critically injured on roads hundreds of miles from a trauma center.
"If you are in some of these areas, you can expect to get the same care you got 40 years ago if you're in a motor vehicle crash," said Ochsner.
Lives that can be saved are only part of the story, said Dr. Arthur Kellermann, chairman of Emory University's Department of Emergency Medicine.
"Disabilities can be averted if we do the right things on the front end," he said.
Political leaders who addressed the gathering could do little more than express concern as the state battles a budgetary crisis. "We know there's a problem there, and we're looking for solutions," said House Speaker Terry Coleman (D-Eastman).
Senate President Pro Tempore Eric Johnson (R-Savannah) urged health care officials to "bring your legislators into your emergency rooms and show them how many physicians are needed."
"This is a basic quality-of-life issue," said Lt. Gov. Mark Taylor. "This is a life-and-death situation for our citizens."
So are the deaths due to bad roads, or bad medical infrastructure? |
Saturday, December 18, 2004
Cure for Yushchenko?
The Blogfather links to a possible antidote for the Ukrainian presidential candidates dioxin problem:Yo-yo diet redistributes toxins in body tissue
Mmmm....tasty! |
The Blogfather links to a possible antidote for the Ukrainian presidential candidates dioxin problem:Yo-yo diet redistributes toxins in body tissue
Perhaps Ukrainian opposition leader Viktor Yushchenko should try an "Olestra diet" to rid his body of dioxin.
It wouldn't be the first time that the "fake fat" product was used as an emergency agent to flush out dioxin, one of a group of chlorinated hydrocarbons that are toxic, lipophilic (attracted to fat) - and persistent in the environment and animal tissues. About five years ago, two Austrian women suffering from dioxin poisoning were given olestra snacks, which resulted in removal of dioxin at 10 times the normal rate, according to some reports.
In an as-yet-unpublished study, researchers at the University of Cincinnati School of Medicine, along with Trevor Redgrave at the University of Western Australia, treated a patient with PCB toxicity over a two-year period with olestra in the form of fat-free Pringles. The patient's chloracne disappeared and the PCB level in fat tissue dropped dramatically.
The same University of Cincinnati School of Medicine team is reporting new research that sheds light into how diet affects retention and re-distribution through the weight gain-loss-regain cycle of chlorinated hydrocarbons, which include DDT, PCBs and dioxins. They also looked at the effects of the additive olestra, which is made by Procter & Gamble, on this redistribution and perhaps more importantly, on excretion of toxins from the body.
Indeed, "combined dietary olestra and caloric restriction caused a 30-fold increase in the rate of excretion" of a test toxin, while the toxin's distribution "into the brain resulting from the restricted diet was reduced by 50% by dietary olestra," the study found.
Mmmm....tasty! |
Thursday, December 16, 2004
The Future of Surgery VI....
In this month's Bulletin of the American College of Surgeons another go-round on the resident work hour limits:Residents and medical students in the 21st century:Better, worse, or just different?. A discussion following a reception for Dr. Donald Palmisano, president of the American Medical Association:
The contrast between then and now is immediately illustrated:
Does that mean that residents today are greedy or uncaring? Or have things changed?:
As Dylan says, "The times they are a'changin'".
In this month's Bulletin of the American College of Surgeons another go-round on the resident work hour limits:Residents and medical students in the 21st century:Better, worse, or just different?. A discussion following a reception for Dr. Donald Palmisano, president of the American Medical Association:
During the informal reception afterward, the discussion turned, as it often does these days, to another perceived crisis in American surgerythe move to the 80-hour workweek and the training of surgery residents in general. As one can imagine, the spectrum of views offered on this subject was diverse, ranging from rebellious to resigned, from uncaring to understanding. Most of the discussants agreed that the current crop of surgery residents is a differentbreed than we were when in training. Of course, we had heard practicing surgeons say the same of us, and, most likely, the current residents will make the same comments about their successors, if they arent already. Nonetheless, we bemoaned the fate of American surgery, reminiscing about surgical training during the previous millennium.One of the authors describes his "groundbreaking" efforts at collective bargaining in 1973
In 1973, the Charity Hospital house staff placed before the administration the following eight demands:
1. A crash cart on every floor. At the time, there was one for the entire hospital.
2. Privacy screens for patients. All patients were, and still are, housed in barracks-style wards.
3. Some sort of cooling system for the patient wards. Not even floor fans were available.
4. Bedside commodes for patients.
5. Air conditioning in the resident call rooms. Residents would sleep on the roof of the hospital, because of the unbearable heat of the New Orleans summer.
6. A place to park.
7. Health care insurance for house staff.
8. A raise of $50 per month, for a monthly of income of $225.
The contrast between then and now is immediately illustrated:
As you may notice, four of these items were directly related to patient care, two were related to working conditions, and only the last two directly affected the residents pocketbooks. To discuss work hours would have been inconceivable, and to discuss lifestyle meant that one actually expected to have a life.
Does that mean that residents today are greedy or uncaring? Or have things changed?:
So what is different today, 30 years and a generation after the demands set forth in 1973? Are the physicians and surgeons of the future more self-centered, demanding to have actual lives while we were content to have jobs? Do the surgeons of the future actually dare to differentiate between having a life and a job, when we thought the two were synonymous? Is it possible that we cared more about our patients, while they care more about themselves? Are we training surgeons or shift workers? Or is it possible that patient care has changed to the point where residents no longer need to fight for patients rights? Are we now finally confronting the fact that one-third of a residents time is spent performing activities with marginal educational value, and that with better communication between physicians and nurses, residents can sleep more and be paged less? Can anyone honestly say that he or she would have preferred less sleep, fewer days off, and less time with their families while in residency, regardless of in which decade it was?That is the unasked question. The "elders" of surgery express concern over the effects the work-week limits will have on patient care and training and are aghast that residents are expressing lifestyle concerns, when they themselves surely cannot offer an honest "yes" to the above question.
As Dylan says, "The times they are a'changin'".
Labels: Future of Surgery
|Tuesday, December 14, 2004
The Creeping Specialty Scourge..
NPR yesterday had a story on the increasing popularity of specialty hospitals and how they are potentially harming the community general hospital:Growing trend of surgeons opening their own specialty hospitals
Mr. Goodwyn continues:
The community hospitals suffer not only because the insured (and more importantly, the healthy insured) are siphoned off to the specialty hospital with the resulting loss of revenue, they may also suffer from medical staff losses. If a physician can accommodate his patients at a specialty hospital or ASC and not need the local community hospital, why would they remain on staff? Sense of community duty? Good manners? For some it is simply an economic decision, and an easy one at that.
|
NPR yesterday had a story on the increasing popularity of specialty hospitals and how they are potentially harming the community general hospital:Growing trend of surgeons opening their own specialty hospitals
MONTAGNE: For patients in many states, planning for certain medical procedures has become more like planning a stay in a hotel. Rather than a traditional hospital, they can choose a specialty surgical hospital. Many of these boutique hospitals are owned by surgeons who refer their own patients. The surgeons can earn income twice on a patient, as a doctor and as a hospital owner. Full-service and community hospitals complain that specialty hospitals are! e threatening their survival by skimming off the most profitable insured surgical patients. Surgeons say small specialty hospitals give patients a better experience. NPR's Wade Goodwyn reports from Baton Rouge.
WADE GOODWYN reporting:
Lafayette and Baton Rouge are in the Cajun heart of fried seafood country.
Unidentified Man #1: You have a bed over there, Hope?
GOODWYN: Catfish, shrimp, etouffe, po' boy sandwiches. In bayou country, the batter is not about baseball, and the oh-so-good food will eventually kill you.
Unidentified Woman: What kind of medical history do you have?
Unidentified Man #2: My daddy had a major heart attack. He died of cerebral hemorrhage.
GOODWYN: The emergency room here at Our Lady of the Lake general hospital is an integral part of this region's health care, its first line of defense. Like many emergency rooms and burn centers and intensive care units, this hospital emergency room is not a moneymaker. It's a money loser.
Mr. BOB DAVIDGE (Our Lady of th e Lake): The question is, how are we going to pay for it? We are losing the ability that we once had.
GOODWYN: Bob Davidge has been Our Lady of the Lake's CEO for the last 25 years.
Mr. DAVIDGE: Every hospital in the country cost-shifts to cover the shortfall in Medicare, Medicaid, charity patients, bad-debt patients. It's all shifted to the private-paying patient. When these facilities focus on just the paying patient, then we lose that ability to cost-shift.
GOODWYN: The facilities that Davidge is talking about are specialty surgical hospitals, and they have begun popping up all over Baton Rouge and Lafayette, six in the last five years. Cardiac surgery, orthopedic surgery, neurosurgery; surgeons are learning here that they can bypass traditional acute-care hospitals and start their own specialty hospitals. But Davidge says that in order for his full-service hospital to stay viable, he needs the surgeons to operate at Our Lady of the Lake, not start their own hospital.
Mr. DAVIDGE: The neuro-hospital that has yet to open, we forecast, will cost to the bottom line $2 1/2 million. That's just about 25 percent of our bottom line from operations. So that's a big, big hit.
Mr. Goodwyn continues:
GOODWYN: Think of these specialty surgical centers as hospitalettes. Most don't have emergency rooms or intensive care units. It used to be that the federal government regulated where and how many new hospitals could be built, but in the mid-1980s, the Reagan administration abolished those laws. Now the national landscape is a hodgepodge of state legislation. Some states still strictly control how many new hospitals are built and what kind of medical services they must offer, but some states have abolished those controls, and it is in these states that specialty hospitals have begun to proliferate: Texas, Oklahoma, Kansas, South Dakota, Arizona and California. And there's been such a rush in Louisiana that some conservative Republican state senators have begun to object.The story goes on to describe the current federal moratorium on specialty hospitals that is due to expire in March of 2005. A study by the Medicare Payment Advisory Commission is ongoing to analyze the impact:
State Senator TOM SCHEDLER (Republican, Louisiana): The last thing I want would be to wake up and find no acute-care hospital in a community with four specialty hospitals. That's a recipe for disaster.
GOODWYN: Tom Schedler represents what is called the North Shore area, from Lake Pontchartrain down to the city of New Orleans. He got involved when his district's general hospital lost 30 percent of its cardiac surgery business after the cardiac surgeons there built their own specialty hospital. That hospital has been such a success that the orthopedic surgeons in Schedler's
For example, they're finding that while full-service hospitals do indeed take a financial hit whenever specialty hospitals open, they usually find ways to recover some of that lost revenue: operating room schedules suddenly become more flexible, turnaround times are shortened, equipment is upgraded.So competition is a good thing. The story also notes that the Medicare reimbursement is the same regardless of where the procedure is performed. The NPR audio also has a useful"summary" of some of the facts surrounding the controversy.
In the last two decades, reimbursement to physicians has been reduced, regulations have increased, malpractice premiums have soared, and the traditional relationships between physicians and hospitals have been drastically altered. Numerous laws and regulations target hospital incentives to physicians, claiming such conduct is "suspect."Virtually any activity that could influence where a physician refers a patient is within the sights of government regulators. The federal government and many states prohibit physicians from referring patients to entities with which the physician, or an immediate family member, has a financial or ownership interest. The federal law, commonly referred to as the "Stark" law, has certain exceptions, including investments in large publicly traded companies, ambulatory surgery centers (ASC) and hospitals as a whole. The theory of the "whole hospital" exception is that there is less risk that profit is the motive for the referral of a patient where the physician's investment bears the financial and regulatory burdens of an entire hospital. In addition, the Stark law acknowledges that profit motives are lessened or eliminated when physicians perform the services on the patients they refer to the ASC or hospital in which they have an ownership interest.Hospitals themselves are beginning to fight back:
Hospitals also have begun to use a more direct tactic, denying or revoking the medical staff privileges to physicians who are in competition with the hospital. Physicians protest this tactic that they call "economic credentialing.' But in 2001, the South Dakota Supreme Court upheld a lower court ruling permitting a general hospital to deny privileges to doctors who were also involved with a local specialty hospital. In Arkansas, six cardiologists who are investors in a heart hospital filed suit against Baptist Health for terminating their medical staff privileges. The hospital argues that it has a responsibility to protect the hospital and to give the public access to a broad range of services; the physicians' competition threatens that. This may be the beginning of a trend. In January, OhioHealth terminated 17 physicians who invested in a nearby surgical hospital, and Eastern Idaho Regional Medical Center terminated the privileges of five physicians who had invested in a multi-surgery facility.That has become an issue in my community as well. A private firm is developing a hospital with some physicians as investors. The new hospital will have an emergency room and care for indigent patients, but I wonder how long the ER would stay open. While the hospital has not threatened to pull outright the privileges of those physicians they have threatened to analyze future payer trends and if the percentage of "private pay" or Medicaid patients they admit to Big Hospital increases after the new facility is opened, they may face sanctions.
The community hospitals suffer not only because the insured (and more importantly, the healthy insured) are siphoned off to the specialty hospital with the resulting loss of revenue, they may also suffer from medical staff losses. If a physician can accommodate his patients at a specialty hospital or ASC and not need the local community hospital, why would they remain on staff? Sense of community duty? Good manners? For some it is simply an economic decision, and an easy one at that.
|
Monday, December 13, 2004
Tales From the Trauma Service II......
Or trauma as chronic disease. 40'ish male pedestrian struck by a motor vehicle. He is "agitated" at the scene with no motor function in his lower extremities. He has no sensation below the nipple. Lax rectal tone, but good motor function of his upper extremities. He has a BAC of 256. Radiographs as follows:

That's going to hurt!! Here is a CT reconstruction:

And for you MRI fans:

And he had an open tibial plateau fracture to boot:


So fairly straightforward case. His FAST exam was negative as was the remainder of his spine films. He began to manifest spinal shock and required a central line and Dopamine. He underwent anterior fusion by the neurosurgeon on HD#2. When I went to the office to put in his charges I discovered that he and the trauma service had crossed paths before.
Two months ago he was admitted for a concussion after a motor vehicle collision. He was intoxicated at that time as well.
Eighteen months ago he was stabbed just below the right nipple. He was found to have a pneumothorax and underwent laparoscopy. A small liver injury was found which had stopped bleeding.
Trauma:the gift that keeps on giving!! |
Or trauma as chronic disease. 40'ish male pedestrian struck by a motor vehicle. He is "agitated" at the scene with no motor function in his lower extremities. He has no sensation below the nipple. Lax rectal tone, but good motor function of his upper extremities. He has a BAC of 256. Radiographs as follows:

That's going to hurt!! Here is a CT reconstruction:

And for you MRI fans:

And he had an open tibial plateau fracture to boot:


So fairly straightforward case. His FAST exam was negative as was the remainder of his spine films. He began to manifest spinal shock and required a central line and Dopamine. He underwent anterior fusion by the neurosurgeon on HD#2. When I went to the office to put in his charges I discovered that he and the trauma service had crossed paths before.
Two months ago he was admitted for a concussion after a motor vehicle collision. He was intoxicated at that time as well.
Eighteen months ago he was stabbed just below the right nipple. He was found to have a pneumothorax and underwent laparoscopy. A small liver injury was found which had stopped bleeding.
Trauma:the gift that keeps on giving!! |
Sunday, December 12, 2004
Sins of Commission....
The Atlanta Journal-Constitution reprinted an opinion piece out of the L.A. Times about the ethical drama surrounding the Governor of Kentucky:Doctor, Reread Your Oath
Dr. Zitrin however, is not merely an impartial observer, as illustrated in this October American Medical News article:
|
The Atlanta Journal-Constitution reprinted an opinion piece out of the L.A. Times about the ethical drama surrounding the Governor of Kentucky:Doctor, Reread Your Oath
A physician is a member of a profession "dedicated to preserving life when there is hope of doing so." That's from the American Medical Assn.'s Code of Medical Ethics. The recent reports of physician participation in prisoner torture in Abu Ghraib and Guantanamo are shockingly reminiscent of Nazi doctors' flagrant violations of the codes of their profession.The AMA's policy may be found here. It reads in part:
But there is another case worth examining, closer to home. On Nov. 8, Kentucky Gov. Ernest S. Fletcher signed a death warrant for convicted murderer Thomas Clyde Bowling, an order later temporarily stayed until the Kentucky courts had more time to consider the issues presented to them. Evidence had been offered that Bowling, who killed two people in 1990, was mentally retarded......Objections flooded his office, and complaints were filed with the Kentucky Board of Medical Licensure, charging him with violating the AMA's ethics code and Kentucky law. The licensure board is expected to consider the matter in January.
The code of the AMA, and of almost every national and international health-related organization, states that physician participation in executions is prohibited. Originally formulated in 1980 and updated in 2000, the AMA principle is clear: A physician should not be a participant in a legally authorized execution, and it defines participation to include an action that could automatically cause an execution to be carried out on a condemned prisoner.
In a case in which the method of execution is lethal injection the method now used in all 38 states with the death penalty the code proscribes any involvement with the procedure, including consulting with or supervising lethal-injection personnel.
Physician participation in an execution includes, but is not limited to, the following actions: prescribing or administering tranquilizers and other psychotropic agents and medications that are part of the execution procedure; monitoring vital signs on site or remotely (including monitoring electrocardiograms); attending or observing an execution as a physician; and rendering of technical advice regarding execution.The policy does not specifically address Governor Fletcher's situation, since it deals with direct physician participation with the actual execution. I agree that a physician shouldn't be the one to push the plunger, but Dr. Zitrin doesn't think that is enough:
In the case where the method of execution is lethal injection, the following actions by the physician would also constitute physician participation in execution: selecting injection sites; starting intravenous lines as a port for a lethal injection device; prescribing, preparing, administering, or supervising injection drugs or their doses or types; inspecting, testing, or maintaining lethal injection devices; and consulting with or supervising lethal injection personnel.
The following actions do not constitute physician participation in execution: (1) testifying as to medical history and diagnoses or mental state as they relate to competence to stand trial, testifying as to relevant medical evidence during trial, testifying as to medical aspects of aggravating or mitigating circumstances during the penalty phase of a capital case, or testifying as to medical diagnoses as they relate to the legal assessment of competence for execution; (2) certifying death, provided that the condemned has been declared dead by another person; (3) witnessing an execution in a totally nonprofessional capacity; (4) witnessing an execution at the specific voluntary request of the condemned person, provided that the physician observes the execution in a nonprofessional capacity; and (5) relieving the acute suffering of a condemned person while awaiting execution, including providing tranquilizers at the specific voluntary request of the condemned person to help relieve pain or anxiety in anticipation of the execution.
Fletcher's legal advisor says the governor did not violate AMA guidelines or other ethical standards in signing the death warrant. Fletcher's role under the law is consistent with the roles of judges fulfilling their legal duty and jurors fulfilling their legal obligations regardless of their professions, he said.Why? I thought the earning of a medical degree made one a physician, not a license to practice. Why should election preclude one to holding a medical license? What if the situation were such that Gov. Fletcher did not sign the death warrant himself, but had the power to commute the sentence? Would his refusal to do so constitute "participation" in an execution? Would physicians who served on juries considering capital cases be liable for sanction if they voted for the death penalty?
But I believe that a physician is not freed of his obligation to comply with his profession's ethical mandates. If Fletcher wanted to forgo that obligation, he should have surrendered his license when he was elected.
Dr. Zitrin however, is not merely an impartial observer, as illustrated in this October American Medical News article:
Arthur Zitrin, MD, is very familiar with this portion of the ethics code. Dr. Zitrin, an 86-year-old retired New York University psychiatrist and self-described death penalty abolitionist, is initiating one of the more controversial attacks on lethal injection. He is identifying physicians who participate in executions in hopes of getting their licenses revoked.So Dr. Zitrin is using the medical board as a political weapon against those that disagree with him. He has filed a complaint against a physician in Georgia for his involvement in executions:
"My effort, and it's been a quixotic effort in some respects, is to identify doctors who participate in executions and work to have charges filed against them for violating medical ethics," Dr. Zitrin said. "It's very hard to identify these doctors. They're paid in cash and the department of corrections won't release their names."
Jim McNatt, MD, medical director for the Georgia board, would not comment on the case specifically but said that this type of complaint was not unique.I wonder how many more complaints will be filed against physicians performing abortions in Kentucky if Governor Fletcher is sanctioned? Others agree that Dr. Zitrin has gone too far:
"The board gets put into political [arguments] all the time in several areas, and we have to look at the facts in each one," he said.
Dr. McNatt said complaints also are filed against doctors who perform abortions but that neither performing abortions nor participating in executions is illegal in Georgia.
New Haven, Conn.-based attorney Kenneth F. Baum, MD, disagrees. "Reasonable people can disagree on the death penalty, and reasonable people can disagree whether physicians should participate," he said. "But it's another thing for one physician to say 'My opinion is right' and to hunt down physicians who are participating in executions and take their licenses away."While the complaint against the Georgia physician may have merit (he personally monitored executions and started a subclavian line in a prisoner who had no peripheral access) the crusade against Gov. Fletcher is silly and demeans the debate at hand.
|
Friday, December 10, 2004
Take A Bite Out of Crime...
This happened just a few blocks from my office:
Must be real desperate to hold up a physician. |
This happened just a few blocks from my office:
Gunman robs doctor leaving his office
A River City doctor was robbed at gunpoint as he left his office Wednesday afternoon, River City police said.
A noted local physician was leaving his office around 5:30 p.m. when a man armed with a handgun approached him, police said in a report.
The gunman stole his wallet and instructed him to get into his BMW to drive him somewhere.
When the gunman attempted to get into the passenger side, Patel drove off. The suspect fired two shots, both of which hit the back of the car.
There were no injuries.
Must be real desperate to hold up a physician. |
Tamoxifen Versus Arimidex....
From the New York Times and The Lancet:Certain Type of Breast Cancer Drug Shows Better Result in Study:
The paper in its' PDF form is here.
Some problems I have with the study:
The usual amplification of benefits provided by relative risk rather than absolute risk. While the absolute benefit of Arimidex over Tamoxifen was about two percent, the relative benefit was 12 percent.
There appears to be no information on staging or indications that there was stage parity between the groups.
The authors were on the payroll of AstraZeneca, the manufacturer of both Tamoxifen and Arimidex. What's the big deal? you may ask, aren't they just robbing Peter to pay Paul? Not exactly:
I report, you decide. |
From the New York Times and The Lancet:Certain Type of Breast Cancer Drug Shows Better Result in Study:
A class of hormone-blocking drugs called aromatase inhibitors was more effective in preventing breast cancer recurrence in women past menopause than was tamoxifen, a medication now prescribed by many doctors, researchers reported yesterday.Here is the summary:
The authors of the study, published online in the British medical journal The Lancet, said the findings suggested that aromatase inhibitors should replace tamoxifen as the first line of treatment for postmenopausal women with breast cancer.
But other experts said it was too early to tell if treating women with aromatase inhibitors from the outset was better than using tamoxifen first, followed by the newer drugs.
The standard adjuvant endocrine treatment for postmenopausal women with hormone-receptor-positive localised breast cancer is 5 years of tamoxifen, but recurrences and side-effects restrict its usefulness. The aromatase inhibitor anastrozole was compared with tamoxifen for 5 years in 9366 postmenopausal women with localised breast cancer. After a median follow-up of 68 months, anastrozole significantly prolonged disease-free survival (575 events with anastrozole vs 651 with tamoxifen, hazard ratio 0·87, 95% CI 0·78-0·97, p=0·01) and time-to-recurrence (402 vs 498, 0·79, 0·70-0·90, p=0·0005), and significantly reduced distant metastases (324 vs 375, 0·86, 0·74-0·99, p=0·04) and contralateral breast cancers (35 vs 59, 42% reduction, 12-62, p=0·01). Almost all patients have completed their scheduled treatment, and fewer withdrawals occurred with anastrozole than with tamoxifen. Anastrozole was also associated with fewer side-effects than tamoxifen, especially gynaecological problems and vascular events, but arthralgia and fractures were increased. Anastrozole should be the preferred initial treatment for postmenopausal women with localised hormone-receptor-positive breast cancer.The greatest benefit was seen in receptor-positive patients for all of the measured outcomes (disease-free survival, time-to-recurrence, time-to-distant-recurrence, overall survival, time to breast cancer death, and contralateral breast cancer). The biggest impact was seen in the reduction of contralateral breast cancer. Arimidex seemed to be more well tolerated than the Tamoxifen.
The paper in its' PDF form is here.
Some problems I have with the study:
The usual amplification of benefits provided by relative risk rather than absolute risk. While the absolute benefit of Arimidex over Tamoxifen was about two percent, the relative benefit was 12 percent.
There appears to be no information on staging or indications that there was stage parity between the groups.
The authors were on the payroll of AstraZeneca, the manufacturer of both Tamoxifen and Arimidex. What's the big deal? you may ask, aren't they just robbing Peter to pay Paul? Not exactly:
About half a million American women use tamoxifen, sold under the brand name Novaldex by AstraZeneca and by other companies in generic form. But a growing body of evidence that aromatase inhibitors can more effectively prevent cancer from returning may have prompted tamoxifen's sales to plummet in recent years. Annual sales of all forms of tamoxifen fell to $52.3 million as of October 2004 from $177.9 million in 2003, according to IMS Health, a pharmaceutical information and health care company.Is there a sinister plot to devalue the drug that is no longer under patent in favor of a branded product?
I report, you decide. |
Thursday, December 09, 2004
Does "Enhancement" Spam Help or Hinder?????
Laptops' heat could hurt men's fertility
For their next project they will do sperm counts on jockey-short wearing bicyclists who use laptops. |
Laptops' heat could hurt men's fertility
Heat generated by the use of laptop computers might affect men's fertility, researchers reported Wednesday.
Using laptops for one hour increased the temperatures of men's scrotums by about 5 degrees, according to a study at State University of New York at Stony Brook.
Earlier studies found that raising scrotal temperatures by more than 2 degrees can decrease the number and quality of sperm, which in turn can reduce fertility.
The new study, published in the European journal Human Reproduction, does not prove laptops affect fertility, since researchers did not measure sperm counts in the 29 volunteers.
For their next project they will do sperm counts on jockey-short wearing bicyclists who use laptops. |
Wednesday, December 08, 2004
The Measuring Stick...
Courtesy of Book of Joe a New Yorker piece by the good Dr. Atul Gawande: THE BELL CURVE. In which Dr. Gawande examines a hospital's soul-baring honesty, and its' struggle to improve. It begins with the diagnosis of cystic fibrosis (CF) in the child that lives near Cincinnati:
Back to online Christmas shopping.
|
Courtesy of Book of Joe a New Yorker piece by the good Dr. Atul Gawande: THE BELL CURVE. In which Dr. Gawande examines a hospital's soul-baring honesty, and its' struggle to improve. It begins with the diagnosis of cystic fibrosis (CF) in the child that lives near Cincinnati:
The one overwhelming thought in the minds of Honor and Don Page was: We need to get to Children's. Cincinnati Children's Hospital is among the most respected pediatric hospitals in the country. It was where Albert Sabin invented the oral polio vaccine. The chapter on cystic fibrosis in the 'Nelson Textbook of Pediatrics"-the bible of the specialty-was written by one of the hospital's pediatricians. The Pages called and were given an appointment for the next morning.The Page family then goes through an intense ordeal with physicians, respiratory therapists and nutritionists. They feel that they are getting the best care possible for their child, but are they?
The one thing that the clinicians failed to tell them, however, was that Cincinnati Children's was not, as the Pages supposed, among the country's best centers for children with cystic fibrosis. According to data from that year, it was, at best, an average program. This was no small matter. In 1997, patients at an average center were living to be just over thirty years old; patients at the top center typically lived to be forty-six. By some measures, Cincinnati was well below average. The best predictor of a CF patient's life expectancy is his or her lung function. At Cincinnati, lung function for patients under the age of twelve-children like Annie-was in the bottom twenty-five per cent of the country's CF patients. And the doctors there knew it.Dr. Gawande then discusses the sparse information about physician outcomes and compares it to the evolution of the CF reporting system that ranks the country's CF treatment centers. What he learns is that clinical pathways and evidence-based protocols do not always a superstar make:
What makes the situation especially puzzling is that our system for CF care is far more sophisticated than that for most diseases. The hundred and seventeen CF centers across the country are all ultra-specialized, undergo a rigorous certification process, and have lots of experience in caring for people with CF. They all follow the same detailed guidelines for CF treatment. They all participate in research trials to figure out new and better treatments. You would think, therefore, that their results would be much the same. Yet the differences are enormous. Patients have not known this. So what happens when they find out?Dr. Gawande then visits the center at Cincinnati Children's, and after some wrangling, visits one of the best, Fairview-University Children's Hospital. What Dr. Gawande finds is that sometimes the vision of one person makes all the difference:
The director of Fairview-University Children's Hospital's cystic-fibrosis center for almost forty years has been none other than Warren Warwick, the pediatrician who had conducted the study of LeRoy Matthews's suspiciously high success rate. Ever since then, Warwick has made a study of what it takes to do better than everyone else. The secret, he insists, is simple, and he learned it from Matthews: you do whatever you can to keep your patients' lungs as open as possible. Patients with CF at Fairview got the same things that patients everywhere did-some nebulized treatments to loosen secretions and unclog passageways (a kind of mist tent in a mouth pipe), antibiotics, and a good thumping on their chests every day. Yet, somehow, everything he did was differentDr. Warick, while accomplishing this, has little regard for "evidence based medicine"
Almost ten per cent of the children at his center get supplemental feedings through a latex tube surgically inserted into their stomachs, simply because, by Warwick's standards, they were not gaining enough weight. There's no published research showing that you need to do this. But not a single child or teen-ager at the center has died in years. Its oldest patient is now sixty-four.Moving along:
The buzzword for clinicians these days is "evidence-based practice"-good doctors are supposed to follow research findings rather than their own intuition or ad-hoc experimentation. Yet Warwick is almost contemptuous of established findings. National clinical guidelines for care are, he says, "a record of the past, and little more-they should have an expiration date.'
We are used to thinking that a doctor's ability depends mainly on science and skill. The lesson from Minneapolis is that these may be the easiest parts of care. Even doctors with great knowledge and technical skill can have mediocre results; more nebulous factors like aggressiveness and consistency and ingenuity can matter enormously. In Cincinnati and in Minneapolis, the doctors are equally capable and well versed in the data on CF. But if Annie Page-who has had no breathing problems or major setbacks-were in Minneapolis she would almost certainly have had a feeding tube in her stomach and Warwick's team hounding her to figure out ways to make her breathing even better than normal.So how do we teach physicians to be like Dr. Warick in an environment that treats medicine as a volume business? Dr. Warick is somewhat of a "maverick" and is willing to try new and different therapies to enhance care. Will physicians locked in to "evidence based" protocols have the ability to "think outside the box"? Since the "technical" aspects of CF care are widely known, if a program can become more aggressive about their care the gap should narrow, shouldn't it? Maybe not:
Don Berwick believes that the subtleties of medical decision-making can be identified and learned. The lessons are hidden. But if we open the book on physicians' results, the lessons will be exposed. And if we are genuinely curious about how the best achieve their results, he believes they will spread.
In the two years since the Cystic Fibrosis Foundation began bringing together centers willing to share their data, certain patterns have begun to emerge, according to Bruce Marshall, the head of quality improvement for the foundation. All the centers appear to have made significant progress. None, however, have progressed more than centers like Fairview.Not exactly a skill that can be taught. So the bell curve is maintained, just shifted to the right. What implications does this have for the rest of us?
"You look at the rates of improvement in different quartiles, and it's the centers in the top quartile that are improving fastest," Marshall says. "They are at risk of breaking away." What the best may have, above all, is a capacity to learn and adapt-and to do so faster than everyone else.
Once we acknowledge that, no matter how much we improve our average, the bell curve isn't going away, we're left with all sorts of questions. Will being in the bottom half be used against doctors in lawsuits? Will we be expected to tell our patients how we score? Will our patients leave us? Will those at the bottom be paid less than those at the top? The answer to all these questions is likely yes.There are always going to be "average" physicians because that's the way that statistics work. The goal of all physicians should be to shrink the distance between "average" and "excellent" to as narrow a range as possible. This is the practical solution since the number of "centers of excellence" may be small, and some conditions are so common, like appendicitis in children that the 13 centers that give the best results would be overwhelmed. Sometimes the difference between "average" and "excellent" is small. And remember, these are statistics, and even "excellent" places have bad outcomes. Some patients, even those with "good insurance" may not have the means to travel to a MD Anderson or Sloan-Kettering. What about them? To sum up:
The hardest question for anyone who takes responsibility for what he or she does is, What if I turn out to be average? If we took all the surgeons at my level of experience, compared our results, and found that I am one of the worst, the answer would be easy: I'd turn in my scalpel. But what if I were a C? Working as I do in a city that's mobbed with surgeons, how could I justify putting patients under the knife? I could tell myself, Someone's got to be average. If the bell curve is a fact, then so is the reality that most doctors are going to be average. There is no shame in being one of them, right?Should we resign ourselves to being "average"? We should strive to improve ourselves, to narrow the gap between "average" and "excellent" so that is insignificant.
Except, of course, there is. Somehow, what troubles people isn't so much being average as settling for it. Everyone knows that averageness is, for most of us, our fate. And in certain matters-looks, money, tennis-we would do well to accept this. But in your surgeon, your child's pediatrician, your police department, your local high school? When the stakes are our lives and the lives of our children, we expect averageness to be resisted. And so I push to make myself the best. If I'm not the best already, I believe wholeheartedly that I will be. And you expect that of me, too. Whatever the next round of numbers may say.
Back to online Christmas shopping.
|
Tuesday, December 07, 2004
Tales From the Operating Room V.....
20-ish postpartum female with several bouts of biliary colic during pregnancy. Set up for cholecystectomy. Liver function tests normal. No jaundice or any other signs of biliary obstruction. Intraoperative picture:
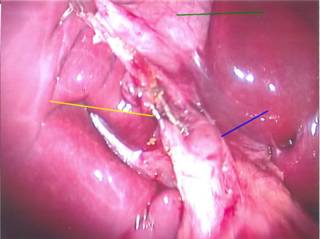
The green line points to the gallbladder, the yellow line to the cystic duct with clips on it and the blue line to the common bile duct, which looked enlarged in my opinion. This picture was taken after the cholangiogram was performed. I perform my cholangiograms with a cystic ductotomy and an Arrow cholangiocatheter. Here are the images:

The proximal system fills well. Yellow line points to the cystic duct. The common duct does not appear to be too dilated.
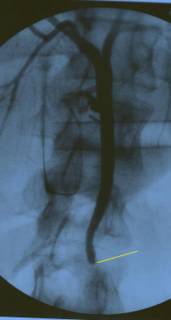
Here's the rub. Normally you would see contrast flowing to the duodenum, indicating the duct was clear. As seen in this study from another patient:
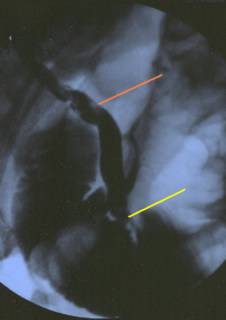
The yellow line shows contrast within the small bowel. The red line shows stones within the common duct.
The differential in this case is: 1) retained common duct stone, 2)malignancy, which would be uncommon in an otherwise healthy 20 year old, and 3)Sphincter of Oddi spasm. The radiographs did not change after administration of glucagon and 20 minutes of breathless anticipation.
This is one of those times that the old "surgical judgment" comes in to play. What to do? Open common bile duct exploration? Laparoscopic ? Both of those are limited by the fact the duct is not that large. Such a duct would be difficult to manipulate and could stricture, causing later trouble. Fortunately I have some excellent gastroenterologists in River City and the patient underwent a successful endoscopic retrograde cholangiopancreatography (ERCP) the next day with a sphincteroplasty. (Sorry, the ERCP pictures aren't very good). Several stones were extracted and she was discharged. |
20-ish postpartum female with several bouts of biliary colic during pregnancy. Set up for cholecystectomy. Liver function tests normal. No jaundice or any other signs of biliary obstruction. Intraoperative picture:

The green line points to the gallbladder, the yellow line to the cystic duct with clips on it and the blue line to the common bile duct, which looked enlarged in my opinion. This picture was taken after the cholangiogram was performed. I perform my cholangiograms with a cystic ductotomy and an Arrow cholangiocatheter. Here are the images:
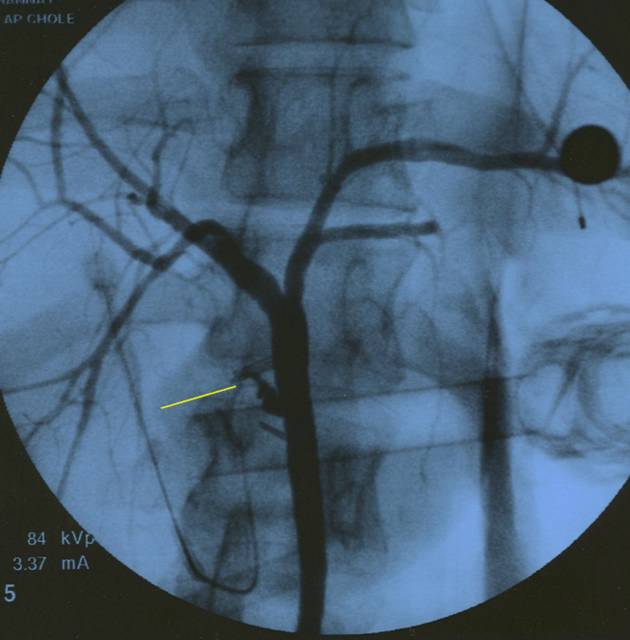
The proximal system fills well. Yellow line points to the cystic duct. The common duct does not appear to be too dilated.

Here's the rub. Normally you would see contrast flowing to the duodenum, indicating the duct was clear. As seen in this study from another patient:
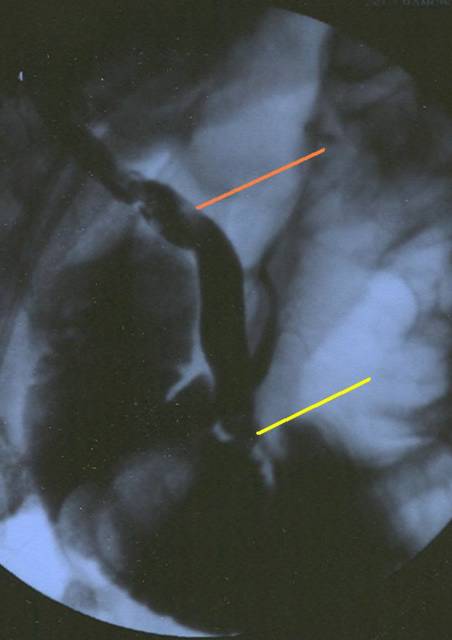
The yellow line shows contrast within the small bowel. The red line shows stones within the common duct.
The differential in this case is: 1) retained common duct stone, 2)malignancy, which would be uncommon in an otherwise healthy 20 year old, and 3)Sphincter of Oddi spasm. The radiographs did not change after administration of glucagon and 20 minutes of breathless anticipation.
This is one of those times that the old "surgical judgment" comes in to play. What to do? Open common bile duct exploration? Laparoscopic ? Both of those are limited by the fact the duct is not that large. Such a duct would be difficult to manipulate and could stricture, causing later trouble. Fortunately I have some excellent gastroenterologists in River City and the patient underwent a successful endoscopic retrograde cholangiopancreatography (ERCP) the next day with a sphincteroplasty. (Sorry, the ERCP pictures aren't very good). Several stones were extracted and she was discharged. |
The Gowns Provide Full Coverage and The Room is Warm...
Visit Grand Rounds XI at The Examining Room of Dr. Charles. |
Visit Grand Rounds XI at The Examining Room of Dr. Charles. |
Wednesday, December 01, 2004
First they Came for the Invalids, and I did not Speak Out.....
Hugh Hewitt asks, "Where is the outrage?" about the "Groningen Protocol" concerning euthanasia of the terminally ill with "no free will". Mr Hewitt links to another article from October of 2004: Euthanasia debate in Europe focuses on children:
Captain Ed points out the danger when the state makes such decisions rather than the family:
Or as Dr. Smith points out, those who do not remember history are doomed to repeat it. |
Hugh Hewitt asks, "Where is the outrage?" about the "Groningen Protocol" concerning euthanasia of the terminally ill with "no free will". Mr Hewitt links to another article from October of 2004: Euthanasia debate in Europe focuses on children:
Four times in recent months, Dutch doctors have pumped lethal doses of drugs into newborns they believe are terminally ill, setting off a new phase in a growing European debate over when, if ever, it's acceptable to hasten death for the critically ill."Experimental policy"? Do they not have Institutional Review Boards in Holland?
Few details of the four newborns' deaths have been made public. Official investigations have found that the doctors made appropriate and professional decisions under an experimental policy allowing child euthanasia that's known as the Groningen University Hospital protocol.
But the children's deaths, and the possibility that the protocol will become standard practice throughout the Netherlands, have sparked heated discussion about whether the idea of assisting adults who seek to die should ever be applied to children and others who are incapable of making, or understanding, such a request.What makes this even more troubling is the decision to euthanize a child may not rest with the parents:
"Applying euthanasia to children is another step down the slope in this debate," said Henk Jochemsen, the director of Holland's Lindeboom Institute, which studies medical ethics. "Not everybody agrees, obviously, but when we broaden the application from those who actively and repeatedly seek to end their lives to those for whom someone else determines death is a better option, we are treading in dangerous territory."
A parent's role is limited under the protocol. While experts and critics familiar with the policy said a parent's wishes to let a child live or die naturally most likely would be considered, they note that the decision must be professional, so rests with doctors.Talk about a slippery slope!
Captain Ed points out the danger when the state makes such decisions rather than the family:
It is one thing for a person to take their own life, or for the family of a brain-dead relative to pull life support. What makes this different is the state apparatus taking on that decision for themselves, deciding who among the citizens supposedly under their protection has no worth and eats up too many resources to go on living. It profoundly repudiates millennia of Western thought, which teaches that individual human life has a precious -- the religious would say sacred -- value.
Without this value at the heart of any society, when humans are valued only for their potential production and devalued for their perceived cost, the decision to end those lives deemed inconvenient to the state comes next. At first, the state limits the killing to those who cases find the broadest acceptance: unborn fetuses, terminally ill patients, and the like. After that threshold has been crossed, the next step is for someone to promulgate a protocol for the state to make the decisions about who lives and who dies. Who becomes inconvenient? The mentally retarded. The insane. The chronically ill, especially those who have incurable communicable diseases.
Or as Dr. Smith points out, those who do not remember history are doomed to repeat it. |
Hard Hat Required II.....
Lots of goodies in the Wall Street Journal this week: Touting Freedom, Bikers Take Aim At Helmet Laws ($):
Lots of goodies in the Wall Street Journal this week: Touting Freedom, Bikers Take Aim At Helmet Laws ($):
Sputnik isn't a typical lobbyist. He has "FREE" tattooed across his forehead, and he wears his hair in a Mohawk. Five earrings dangle from his left ear. But statehouse veterans in Texas have taken the 66-year-old motorcycle activist seriously ever since he led a successful campaign in 1997 to repeal that state's mandatory helmet law.The lobbying efforts are soon to increase as state legislatures begin to meet next month. We have fallen down on the job somewhat here:
Sputnik (his legal name) and other unlikely biker-lobbyists like him are fighting, state-by-state, for what they see as freedom on the road. Many other people see it as an assault on safety and common sense.
Over nearly three decades, bikers have pushed successfully to weaken or eliminate helmet laws in 29 states. Most of that activity came in the 1970s, but recently, bikers have been active again. Since 1997, five states, including Texas, have repealed laws requiring all motorcycle riders to wear helmets. The other four are Florida -- which, like Texas, is a major biker haven -- and Pennsylvania, Kentucky and Arkansas. Federal statistics show that, on average, in the years after the recent legislative changes, helmet use dropped, and motorcycle deaths increased.
To some, the retreat from helmet requirements, led by a vocal minority of riders, defies logic. John Morris, head of the trauma center at Vanderbilt University Medical Center in Nashville, Tenn., says he sees "on a regular basis individuals who don't go home because they didn't wear a helmet." But until recently, doctors groups hadn't made a priority of countering the increasingly savvy biker-activists. For varying reasons, a range of constituencies that might be expected to oppose the helmet-free bikers haven't done so very aggressively, or at all........Here is the editorial with an accompanying Statement in support of motorcycle helmet laws:
......The helmet debate doesn't have a victims group similar to Mothers Against Drunk Drivers, and trauma surgeons are only now mobilizing in earnest. The Journal of the American College of Surgeons, which is sent to the group's 60,000 members, published an editorial in its August issue titled, "Motorcycle Helmet Laws: Every Surgeon's Responsibility." M. Margaret Knudson, one of the authors and chair of the group's committee on injury prevention, says in an interview that doctors have a "duty, really, to make our senators and congressman aware of the value of wearing a helmet."
Total care of the trauma patient includes endorsement of measures designed to prevent injuries. Regarding the use of motorcycle helmets, the American College of Surgeons recognizes that:Many states are now paying the price for repealing those laws:
Helmeted motorcycle riders have up to an 85 percent reduced incidence of severe, serious, and critical brain injuries compared with unhelmeted riders.
Unhelmeted motorcyclists are over three times as likely to suffer a brain injury when compared with helmeted motorcyclists.
The average inpatient care costs for motorcyclists who sustain a brain injury are more than twice the costs incurred by hospitalized motorcyclists without brain injury.
A large portion of the economic burden of motorcycle crashes is borne by the public.
In states with universal helmet use laws, helmet use is close to 100 percent.
When universal helmet use laws are enacted, helmet use increases and fatalities and serious injuries decrease.
When universal helmet use laws are repealed, helmet use decreases and injuries and associate costs increase.
Therefore, the American College of Surgeons supports efforts to enact and sustain universal helmet laws for motorcycle riders.
In the six years since Texas repealed its law in 1997, the annual rate has jumped nearly 30%, to an average 10.95 deaths per 10,000 registered motorcycles, compared with an average of 8.46 deaths for the two years prior to the repeal. In Kentucky, the average rate has jumped to 9.9 in the five years since its 1998 repeal, up 55% compared with the average for the two years before.Georgia has the distinction of passing the first helmet law in 1962. Some states, such as Florida require additional insurance if a rider wishes to go without a helmet. Such policies are for such low amounts ($10,000) that they can be consumed within hours of the injury, and come nowhere close to paying long-term costs. The struggle of a libertarian physician continues..... |
In Florida, in the three years since repeal, the rate is up 21%, to 8.94, compared with the two-year average prior to the repeal. Last year, 358 motorcyclists died in Florida. That is just 10 fewer deaths than occurred in California, the largest motorcycling state, which has 43% more registered motorcycles than Florida. California has a mandatory helmet law.
Nationally, motorcycle deaths rose 12% in 2003, to 3,661. That is the sixth straight year motorcycle deaths have risen. Twelve percent is the largest annual increase since 1988. The national fatality rate increased 4.4%, to 6.82 deaths per 10,000 motorcycles, the highest such figure since 1990. That rate is four-and-a-half times as high as the auto-fatality rate.
The jump in motorcycle deaths in 2003 came in a year when total highway fatalities dropped, federal statistics show. Alcohol-related fatalities fell 3%, to 17,013, and deaths of passengers not wearing seatbelts fell 6.5%, to 18,019. Federal officials attribute those declines to states passing tougher seatbelt and drunk-driving laws.
![]()





