Friday, October 13, 2006
Tales from the Trauma Service XVI.....
Patient shot in the back at unknown range. Allegedly with a .223 caliber round. Here is the initial x-ray:
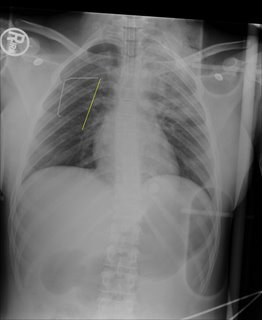
The yellow line (and paperclip) indicates the entry wound on the patient's back. Now as for the exit, that will be revealed shortly. Here are some additional images:
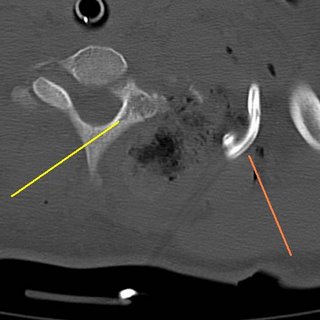
The yellow line represents a lamina fracture of the first thoracic verterbra. No hints on what the green line points to.
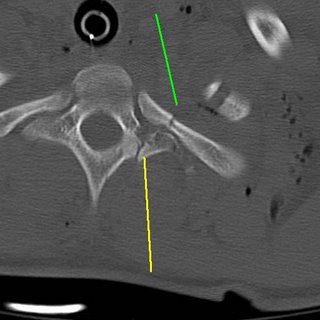
Transverse process fracture (yellow) and an associated rib fracture (green).
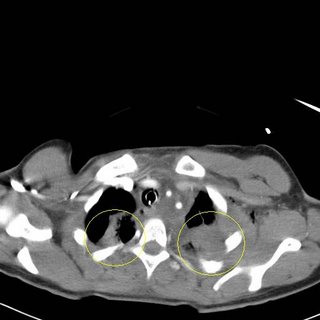
Bilateral pulmonary contusions, left greater than right. There is also some blood in the left hemithorax.
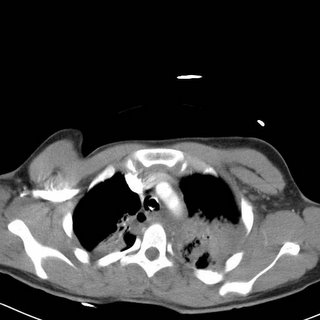
The contusions continue. Now for what you have been waiting for:
WARNING, POTENTIALLY OFFENSIVE IMAGES FOLLOW:
The brachial plexus. Here is some of the anatomy of the area:
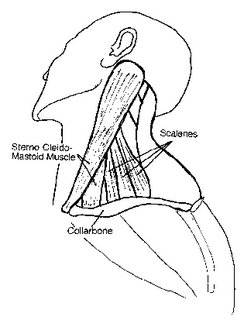
From this diagram we can see the scalene muscles which lie posterior to the SCM. Those were pretty much destroyed by the blast. This next diagram

The brachial plexus also lies here. The phrenic nerve (which controls the diaphragm) does too. Prior to intubation the patient had no motor or sensory function of their left arm. We will probably obtain an EMG next week.
Patient shot in the back at unknown range. Allegedly with a .223 caliber round. Here is the initial x-ray:

The yellow line (and paperclip) indicates the entry wound on the patient's back. Now as for the exit, that will be revealed shortly. Here are some additional images:

The yellow line represents a lamina fracture of the first thoracic verterbra. No hints on what the green line points to.
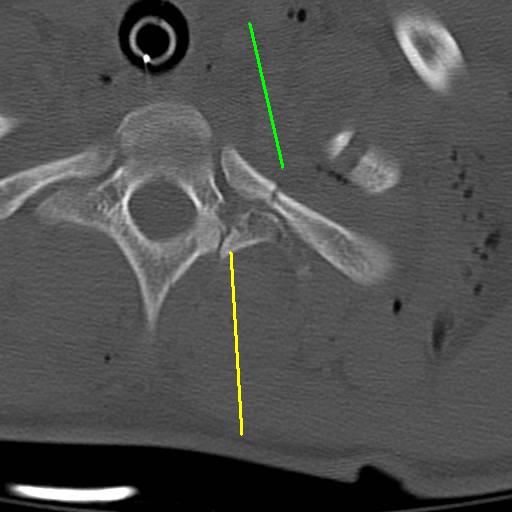
Transverse process fracture (yellow) and an associated rib fracture (green).
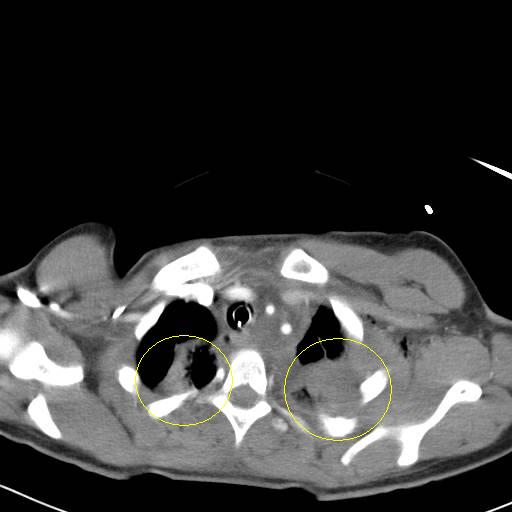
Bilateral pulmonary contusions, left greater than right. There is also some blood in the left hemithorax.
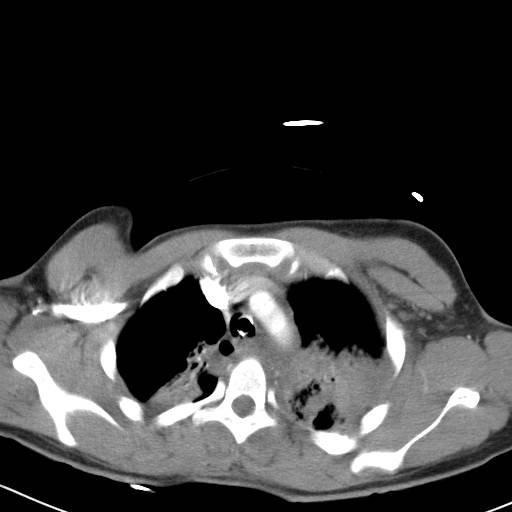
The contusions continue. Now for what you have been waiting for:
WARNING, POTENTIALLY OFFENSIVE IMAGES FOLLOW:
YOU HAVE BEEN WARNED!!!
Here is the exit on the anterior neck:
With a 6cc syringe for comparison:

The structure at the anterior of the wound is the posterior border of the sternocleidomastiod (SCM) muscle. I was able to digitally explore the wound and able to palpate inferior to the fractures seen in the CT scans above. Bleeding was primarily from fractured bone and torn muscle. No injury of the carotid, jugular vein, esophagus or trachea was seen. The wound was irrigated, packed with gelfoam and surgicel and I placed a Jackson-Pratt drain (that's what the green line was indicating).
But something very important does live there:
The brachial plexus. Here is some of the anatomy of the area:

From this diagram we can see the scalene muscles which lie posterior to the SCM. Those were pretty much destroyed by the blast. This next diagram

The brachial plexus also lies here. The phrenic nerve (which controls the diaphragm) does too. Prior to intubation the patient had no motor or sensory function of their left arm. We will probably obtain an EMG next week.
Labels: Tales from the Trauma Service
|![]()





