Wednesday, December 22, 2004
Don't Let Me Touch Your Breasts....
As they likely will have cancer. Three women over the past five weeks:
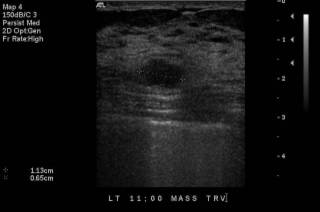
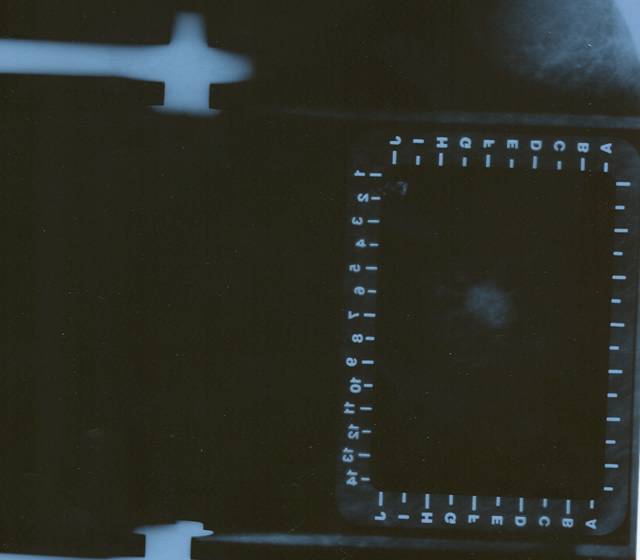
70-ish female with a several year history of breast mass, but was "afraid" to have it evaluated. Only went to the doctor when it became painful and her nipple retracted. She was too tender to have a mammogram. In office ultrasound:
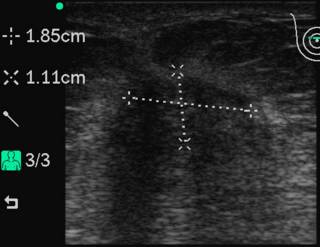
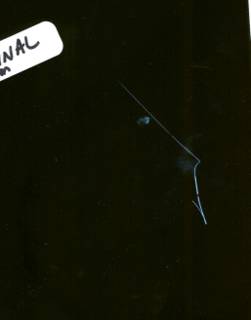
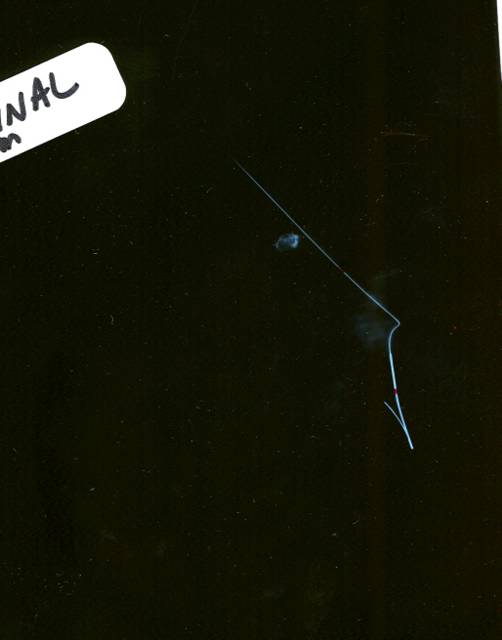
With a Sonosite 180, this is the transverse view. We then went to a core biopsy:
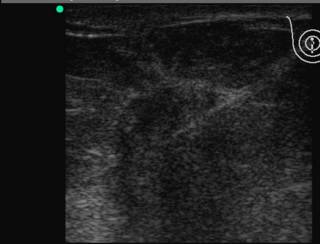
The white line is the needle. It was positive for invasive lobular cancer. She elected to have a mastectomy. She had the only enlarged level III nodes I have encountered in my career. 19 out of 20 nodes were positive. Ignorance is not always bliss.
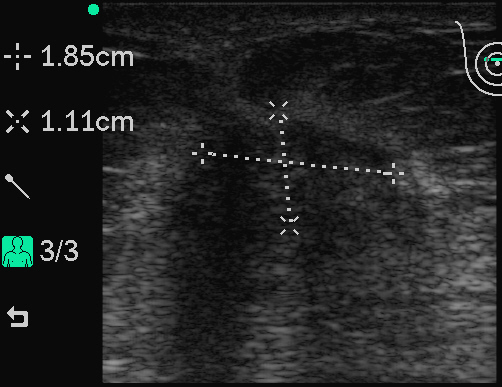
40-ish with a newly-discovered mass. She was seen by another physician who sent her to the radiologist for a core biopsy:
The core biopsy revealed "stromal fibrosis". One of the disadvantages of core biopsy is the possibility of sample error. If the path report doesn't agree with the clinical scenario, don't trust it. She underwent an open wire-localized biopsy which revealed invasive cancer. She chose breast conservation. Her lumpectomy specimen had DCIS within it, not seen on earlier biopsies. Had I known this I may have tried to steer her toward mastectomy and reconstruction, given the increased chances of recurrence. The post-lumpectomy radiation will help take care of it.
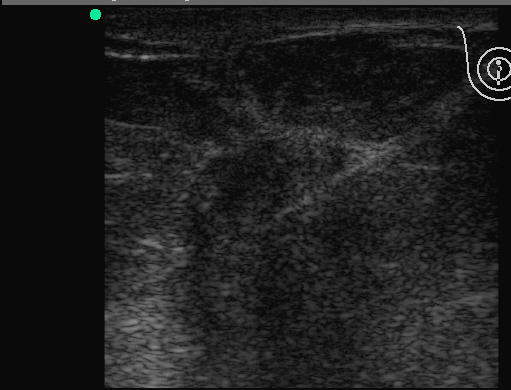
Lastly a 60-ish woman with an abnormal mammogram, unfortunately her diagnostic films did not scan well, but her compression and localization films did:
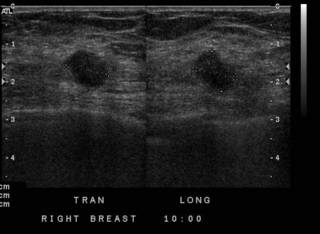
Here is the ultrasound:

She opted for excisional biopsy. Yet again, a malignant diagnosis. She opted for a mastectomy, scheduled for the Monday after Christmas. |
As they likely will have cancer. Three women over the past five weeks:
70-ish female with a several year history of breast mass, but was "afraid" to have it evaluated. Only went to the doctor when it became painful and her nipple retracted. She was too tender to have a mammogram. In office ultrasound:
With a Sonosite 180, this is the transverse view. We then went to a core biopsy:
The white line is the needle. It was positive for invasive lobular cancer. She elected to have a mastectomy. She had the only enlarged level III nodes I have encountered in my career. 19 out of 20 nodes were positive. Ignorance is not always bliss.
40-ish with a newly-discovered mass. She was seen by another physician who sent her to the radiologist for a core biopsy:

The core biopsy revealed "stromal fibrosis". One of the disadvantages of core biopsy is the possibility of sample error. If the path report doesn't agree with the clinical scenario, don't trust it. She underwent an open wire-localized biopsy which revealed invasive cancer. She chose breast conservation. Her lumpectomy specimen had DCIS within it, not seen on earlier biopsies. Had I known this I may have tried to steer her toward mastectomy and reconstruction, given the increased chances of recurrence. The post-lumpectomy radiation will help take care of it.
Lastly a 60-ish woman with an abnormal mammogram, unfortunately her diagnostic films did not scan well, but her compression and localization films did:
Here is the ultrasound:


She opted for excisional biopsy. Yet again, a malignant diagnosis. She opted for a mastectomy, scheduled for the Monday after Christmas. |
![]()





