Tuesday, September 28, 2004
More Tales From the Operating Room.....
Teenaged male presents with three day h/o severe abdominal pain. Crampy in nature and it awoke him from sleep. Positive for nausea and vomiting. No BM since onset of pain. Admitted to the hospital by his pediatrician. WBC at that time was 12 with 90 neutrophils, no segs. His glucose is elevated. Abdominal film obtained:

His symptoms do not improve. A hemoglobin A1C is obtained and is 6.4. A sed rate today is 4. A CT scan of his abdomen and pelvis is obtained today:
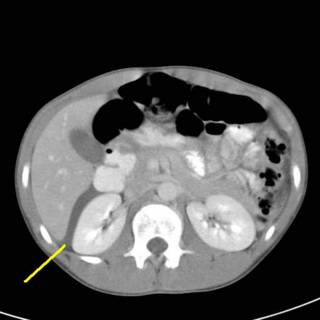
Fluid seen in Morrison's pouch. His pancreas is enlarged according to the radiologist.

Now we see some dilated small bowel loops and more fluid.
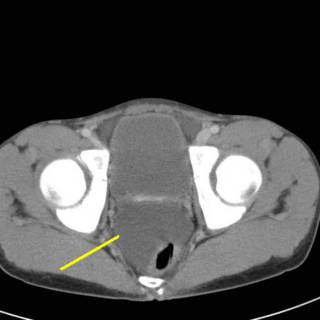
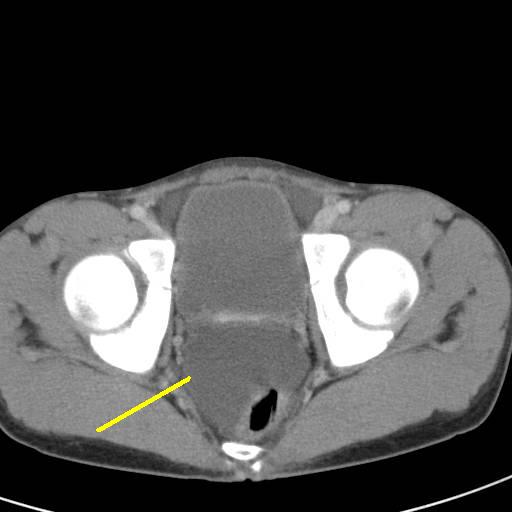
Fluid in the pelvis which has displaced his rectum.
I am asked to see this patient. He is very uncomfortable. His abdomen is distended with diffuse guarding. He is thin and muscular so that is not surprising. His bowel sounds are very faint. He really doesn't have any rebound. His urine is clear. His alkaline phosphatase, amylase, and lipase are all normal. This patient doesn't really add up to me. I obtain another CBC and while his WBC's are now 9, he has a left shift. I have mentioned the "sleep test" before, and I just could not imagine sleeping well tonight if I sat on this kid. Sometimes it is best to "operate first and ask questions later".
Let's take a look.....
WARNING! WARNING!!! The following images may be offensive!!!

O.K. YOU HAVE BEEN WARNED!!!

Here is what I found. The black line points to the cecum, the yellow line to the terminal ileum and the red line to what appears to be a Meckel's diverticulum.

Just to give you an idea of size. I wear 81/2 gloves.
I bathed it in warm saline, I stared at it hard and spoke lovingly to it. I had the CRNA give the patient an ampoule of fluorescein and did a Wood's lamp exam. The black area unsurprisingly did not light up. The amount of small bowel was about 2 feet. If any of the ischemic bowel had lit up at all I would have done a limited resection and come back for a second look in 24 hours. But given its' appearance, I did not think there was much to be gained from that.

Here is the ex vivo specimen. You can see the band that served as the axis of the volvulus. 35 percent of Meckel's diverticula (MD) present with obstruction.
MD is often called the "condition of twos". It is twice as common in males, contains two types of tissue (gastric and pancreatic), usually two inches long, occurs within two feet of the ileocecal valve, and occurs in 2 percent of the population. MD is often confused for appendicitis.
This is the first MD I have encountered, it was truly memorable. |
Teenaged male presents with three day h/o severe abdominal pain. Crampy in nature and it awoke him from sleep. Positive for nausea and vomiting. No BM since onset of pain. Admitted to the hospital by his pediatrician. WBC at that time was 12 with 90 neutrophils, no segs. His glucose is elevated. Abdominal film obtained:

His symptoms do not improve. A hemoglobin A1C is obtained and is 6.4. A sed rate today is 4. A CT scan of his abdomen and pelvis is obtained today:

Fluid seen in Morrison's pouch. His pancreas is enlarged according to the radiologist.

Now we see some dilated small bowel loops and more fluid.
Fluid in the pelvis which has displaced his rectum.
I am asked to see this patient. He is very uncomfortable. His abdomen is distended with diffuse guarding. He is thin and muscular so that is not surprising. His bowel sounds are very faint. He really doesn't have any rebound. His urine is clear. His alkaline phosphatase, amylase, and lipase are all normal. This patient doesn't really add up to me. I obtain another CBC and while his WBC's are now 9, he has a left shift. I have mentioned the "sleep test" before, and I just could not imagine sleeping well tonight if I sat on this kid. Sometimes it is best to "operate first and ask questions later".
Let's take a look.....
WARNING! WARNING!!! The following images may be offensive!!!
O.K. YOU HAVE BEEN WARNED!!!

Here is what I found. The black line points to the cecum, the yellow line to the terminal ileum and the red line to what appears to be a Meckel's diverticulum.

Just to give you an idea of size. I wear 81/2 gloves.
I bathed it in warm saline, I stared at it hard and spoke lovingly to it. I had the CRNA give the patient an ampoule of fluorescein and did a Wood's lamp exam. The black area unsurprisingly did not light up. The amount of small bowel was about 2 feet. If any of the ischemic bowel had lit up at all I would have done a limited resection and come back for a second look in 24 hours. But given its' appearance, I did not think there was much to be gained from that.

Here is the ex vivo specimen. You can see the band that served as the axis of the volvulus. 35 percent of Meckel's diverticula (MD) present with obstruction.
MD is often called the "condition of twos". It is twice as common in males, contains two types of tissue (gastric and pancreatic), usually two inches long, occurs within two feet of the ileocecal valve, and occurs in 2 percent of the population. MD is often confused for appendicitis.
This is the first MD I have encountered, it was truly memorable. |
![]()





