Thursday, January 13, 2005
The Future of Surgery IX...
Another article from General Surgery News:Initiatives Being Considered To Offer 'More Efficient' Track to Specialization:
The Powers That Be in surgery have examined this as well. In the latest Annals of Surgery:American Surgical Association Blue Ribbon Committee Report on Surgical Education: 2004:

Certainly more complicated than the current "cylindrical" or "pyramid" programs of today. Given that surgeons are some of the most dogmatic of physicians out there, if even some of this comes to fruition it will be amazing.
Another article from General Surgery News:Initiatives Being Considered To Offer 'More Efficient' Track to Specialization:
The American Board of Surgery (ABS) recently proposed the creation of a six-year primary certificate in vascular surgery, which represents the first time the board will offer a primary certificate that does not require prerequisite training and certification in general surgery. The proposal is under consideration by the initial review group of the American Board of Medical Specialties, and a decision on whether to proceed with the program is expected by the middle of next year.This is not a small move, according to a member of the American Board of Surgery:
Leaders in the fields of cardiac, breast and emergency/trauma surgery are also discussing focused training pathways, the result of a loud and growing clamor for more such specialty programs driven by factors such as the unwillingness among doctors today to train for many years, particularly female doctors, who will form an estimated 60% to 70% of the medical student body within 20 years. Currently, fully 70% of general surgery trainees eventually opt to undergo subspecialty training, and most do so by taking one to three years of fellowship training after a five-year general surgery residency. As a precedent, plastic surgery has a variety of training options, not all of which require completion of a general surgery residency.
"We need to recognize the fact that we are going to continue to need surgeons, and we have to ensure that our training programs and surgical careers are attractive to students of both genders," ABS chair Barbara Bass, MD, told General Surgery News. "We have to meet the surgical workforce needs of America, and to do that we have to come up with more efficient training pathways, albeit deliberately and thoughtfully and without sacrificing quality, or we're not going to have enough surgeons."One of those who disagree:
Dr. Bass described the decision to consider a primary certificate in vascular surgery as "a huge step, almost earthquaky" for the ABS. And the tremors have already extended to surgeons across the country, creating a huge fissure between approximately equally sized camps of those who support a continued move to reduced training time for specialists, and those who feel it may spell disaster for surgery.
For example, Gary Hoffman, MD, a colorectal and general surgeon who operates at Cedars-Sinai Medical Center in Los Angeles, is incensed by the impetus to create a variety of specialty surgical certificates.But the handwriting is on the wall and is difficult to scrub off:
"The surgeons in whose hands we now place our lives have had to spend a necessary five years learning the craft of surgery. That is why four-year general surgical residencies were eliminated years ago," Dr. Hoffman said. "What would be the ostensible purpose of even providing any general surgical training to specialty surgeons---to learn to tie a few surgical knots or to know when to place a nasogastric tube? ... This proposed lowering of our standards to fit our lifestyles may simply be a mirror of a bigger societal picture. For that analysis, however, you will need to consult a philosopher or historian. From my end of the scalpel, surgical training in all specialties needs to be strengthened, not weakened."
But Henry Kuerer, MD, who heads the Breast Surgical Oncology Training Program at M.D. Anderson Cancer Center in Houston, supports it. He holds up the plastic surgery program at Baylor College of Medicine as a shining example of a successful shortened specialty program. Residents in the Baylor program complete three years of general surgery and then three years of plastic surgery training under Saleh Shenaq, MD, professor and chief of the Division of Plastic Surgery in the Michael E. DeBakey Department of Surgery. Dr. Kuerer sees it as an excellent model for the development of similar training programs in breast surgery and other specialties.Patient demand, dear reader, will be the straw that stirs the drink not only of increased surgical specialization but of increased specialization of medicine as a whole. Some other opinions:
"We train Dr. Shenaq's residents at the third-year level in oncologic surgery and we have found them to be very, very good, and a pleasure to work with," Dr. Kuerer told General Surgery News. "My feeling is that a breast surgeon could have three years of general surgery and three years of breast oncology, which would include rotations on the multidisciplinary care of breast patients, including radiation, medical oncology, breast imaging, plastic surgery and clinical research skills."
Dr. Kuerer says patient demand is one of the seismic forces shaping this debate, as consumers become more savvy and increasingly demand treatment by breast specialists, which is making the ground tremble under the feet of some general surgeons.
"The general surgeons are concerned that even though they have appropriate surgical training and take care of breast problems, they may be shut out because patients might insist on having 'expert' surgeons with specialty training," noted Dr. Kuerer.(emphasis mine)
Others see truth to both sides of the argument. Brian Bansidhar, MD, colon and rectal surgical fellow, Lehigh Valley Hospital, Allentown, Pa., agrees that reducing the amount of general surgical training would still create specialists who are competent surgeons. However, he feels that experience outside of one's specialty area helps produce a more well-rounded surgeon.Best of luck to Dr. Bansidnar if he tries to "initiate the right treatment" without consulting an orthopedist. He and his liability carrier may need it.
"Just as an example, in my residency, we spent a month and a half doing orthopedic surgery," he said. "Did I have to do that? No. Am I going to be doing any orthopedic surgery throughout my career? No. But what that exposure did was to allow me to take trauma and general surgical patients who had orthopedic injuries, and see the big picture. Surgical issues aren't neatly compartmentalized; one problem will affect another. That being said, now I can at least better see some of the nuances and subtleties of the orthopedic injuries and initiate the right treatment, as opposed to saying, 'Well, just call orthopedics, I don't know what to do.' To say that would not be the right thing to do, nor would it be the best thing for the patient."
Kimberly Van Zee, MD, associate attending surgeon, Memorial Sloan-Kettering Cancer Center, New York City, also sees the need for a difficult, fine-linebalancing act.Dr. Van Zee's first point is taken up well by this commenter to a previous post. But the second is also valid. The number of certain cases are finite as is the hours residents are allowed to work. If proficiency is to be maintained, some early specialization will need to be allowed.
"Less exposure to general surgery would result in the surgical subspecialist being less able to treat or recognize signs or symptoms of a disorder outside of [his or her] subspecialty," she said, recognizing one argument for not changing the current training system. "But as resident work hours decrease, and the clinical experience obtained during the five-year general surgery residency decreases, an argument in favor of the earlier split arises: those who are going to continue in general surgery would be the beneficiaries of having fewer colleagues to share a limited number of the more unusual cases, thereby allowing them to complete their training with more experience."
The Powers That Be in surgery have examined this as well. In the latest Annals of Surgery:American Surgical Association Blue Ribbon Committee Report on Surgical Education: 2004:
American surgical education has a rich heritage, and its programs produce some of the best trained and most competent surgeons. Although surgery residency training has changed little since its formulation by Halsted at the beginning of the last century, surgery residency and fellowship programs continue to maintain high standards because they are highly structured, monitored, evaluated, and credentialed.The paper contains recommendations concerning medical workforce, medical student and resident education, resident workhours, faculty and professional development, and research support. The panel has the following to say about the structure of residency training:
At the dawn of the 21st Century, however, numerous forces for change are impacting medical education in general and surgical training in particular. On the one hand, the explosion of knowledge from the advances of science, systems, and information technology provide new opportunities to improve our training programs. On the other hand, as the public has become increasingly better informed about its healthcare needs and safety, its expectation has shifted and now increasingly demands advanced and specialized care. Contrary to earlier predictions of excess physicians by 2010, we appear to be on the threshold of a shortage in physician workforce. This impending shortage should be viewed in the context of Association of American Medical Colleges (AAMC) data, which show that the number of applicants to medical schools in the United States has declined by 25% since 1996. Now, nearly 50% of students entering medical school are women. The average U.S. medical student now graduates with a debt in excess of $100,000. Students of both genders are increasingly selecting specialties with more controllable lifestyles than general surgery. Furthermore, general surgery residencies experience an attrition rate of nearly 20%, primarily because of lifestyle concerns of residents. Major changes have occurred and more are foreseen in the practice of surgery. Much clinical care has moved from the inpatient hospital setting to the outpatient, and the length of stay for inpatients has significantly decreased. These shifts have resulted in a significant impact on both undergraduate and graduate medical/surgical education. Surgical care is moving from discipline-based to disease-based practice in which surgeons will increasingly practice within a team of experts. How do we train surgeons to be leaders of such multidisciplinary teams?
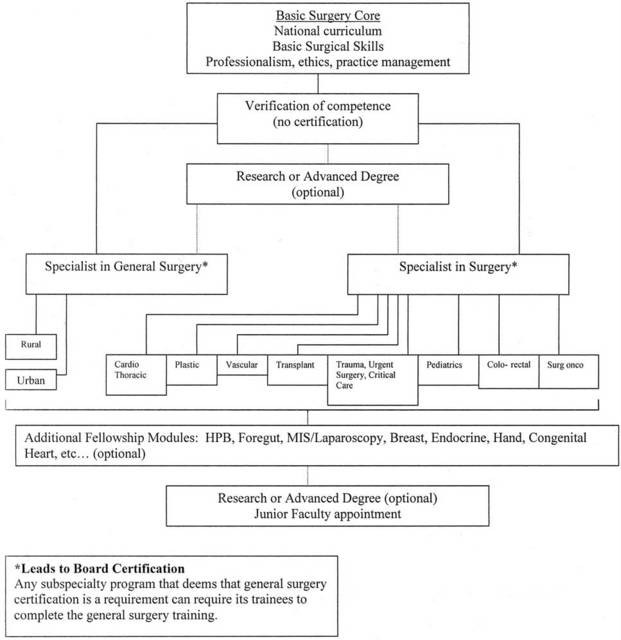
There are many forces driving change in the nature and structure of surgical residencies. Among these are the explosion of knowledge in all surgical fields; new technologies for teaching and assessing surgical skills and for performing surgery; evolution toward multidisciplinary collaborations in patient care; progressive subspecialization; concern for quality and safety of patient care; emphasis on professionalism and competency; and higher expectations of patients. Regulatory changes have limited allowable work hours by residents and put additional stress on the ability to meet the service needs of hospitals as educational needs are given priority.To that end the authors put forth a suggested structure of training that looks like an organizational chart for a government bureaucracy:
Today's surgical resident is a different person. There are more women in surgical training, and residents have more education-related debt. Residents have greater concerns about their lifestyle and length of training. There is need to maximize efficiencies and minimize the duration of residency.
It is increasingly apparent that as subspecialization in surgery continues to evolve and the appeal of broad general surgical practice diminishes, the illusion that a uniform training program purporting to produce competence in all areas is fading. One size no longer fits all. Uncommon case materials are less efficiently distributed when they are used to train individuals whose ultimate goals do not involve focus in these areas. Education research is pushing toward competence-based advancement, replacing time-in-service.
Subspecialty fellowship training is at present largely unregulated, unsupervised, nonuniform, and uncertified. Research by residents during residency is too often for the sole purpose of attaining a clinical fellowship or to meet the needs of faculty for laboratory workers.
A new paradigm is needed that promotes both the varieties of general surgical practice and the subspecialties that derive from general surgery. This training paradigm must achieve greater efficiency and use different methods to be able to accommodate the changing needs of surgical residents and surgery as it will be practiced.
Recommendations
1. Surgical residencies should be restructured to ensure that all trainees receive a common grounding in basic principles of surgical disease and patient care.
2. There needs to be acceptance of the reality that most surgeons will confine the scope of their practices to meet definable goals. This should lead to earlier differentiation into goal-oriented specialty tracks.
3. New teaching technologies (ie, simulators, virtual reality) and verification of competence at each training milepost should be introduced as they become validated and available. A goal should be to define a curriculum for surgical skills that must be acquired by surgical trainees outside the operating room before they begin to operate on patients.
4. It is suggested that a modular format be developed to include a basic surgical core curriculum, and further training in either general surgery or a surgical subspecialty leading to the relevant, specific certification.
5. Furthermore, focused subspecialization would be available through postgraduate fellowships (ie, breast, endocrine, HPB, congenital heart, hand).
6. An optional research module of not less than 2 years can either be interposed between the basic and advanced modules or taken at completion of the residency/fellowship for career development in conjunction with a first faculty position.
7. The option to study for completion of an advanced graduate degree (PhD, MPH, MBA) may occur either after the basic module or after residency.
8. Design, supervision, and certification of the new curricula and the training programs in which they will be used will remain the domain of the respective Boards, RRCs, and surgical specialty societies.
9. It is understood that there will be manifold logistic challenges to implementation, including acceptance by the various stakeholders
(emphasis mine)
Certainly more complicated than the current "cylindrical" or "pyramid" programs of today. Given that surgeons are some of the most dogmatic of physicians out there, if even some of this comes to fruition it will be amazing.
Labels: Future of Surgery
|![]()





