Friday, March 18, 2005
Tales from the Trauma Service VII...
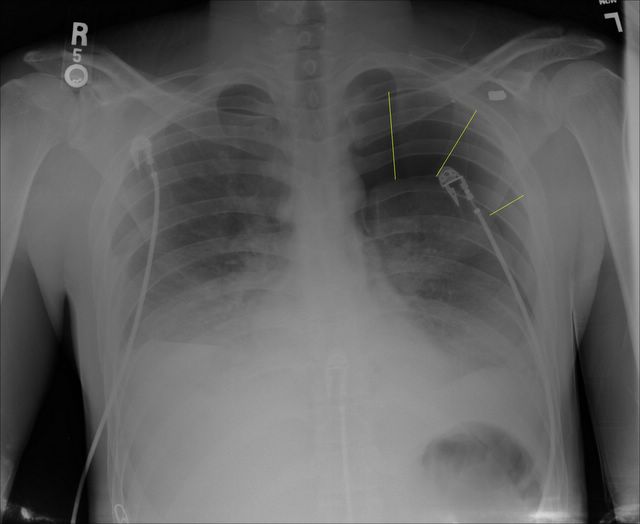
Sometimes millimeters make the difference. 20-ish year old shot in the right side of his back. He was tachycardic at the referring facility, but otherwise stable. No chest tubes were placed. Here is his initial CXR:
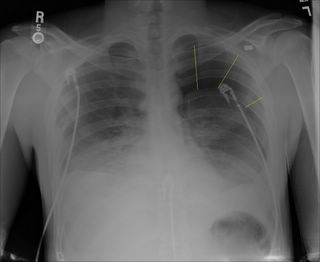
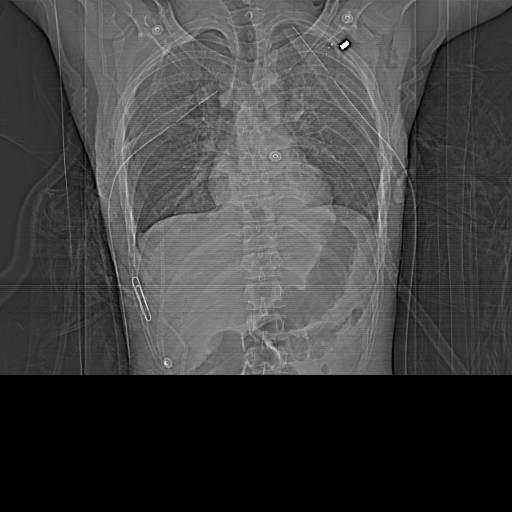
Interestingly the left pneumothorax and the bullet in the left side of his chest was not mentioned during the presentation. A better view (with some chest tubes) can be seen in the scout film of his CT:
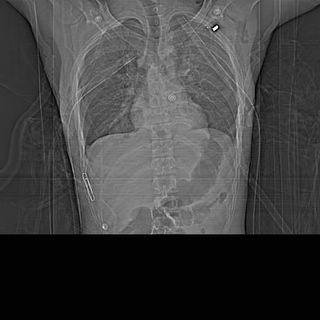
A paperclip marks the entry wound. Lots of vital things live between point "A" and point "B". Since he was hemodynamically stable he could undergo a complete radiographic evaluation instead of an exploration. After discussion with the radiologist he underwent a CT angiogram of his chest rather than a conventional angiogram:
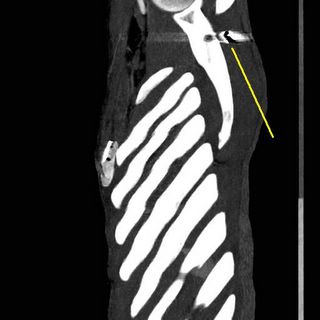
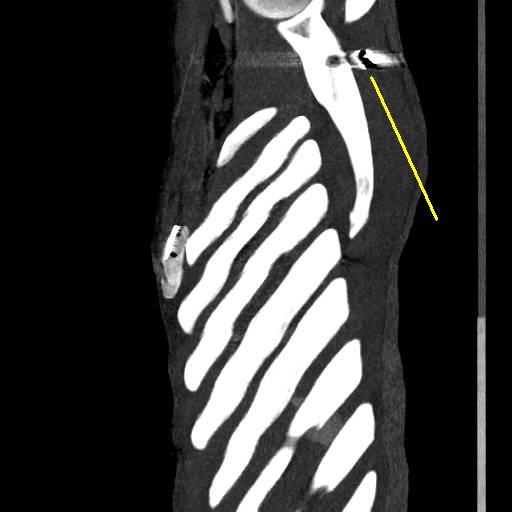
This is one of the leftmost slices of the reconstruction showing the projectile posterior to the left scapula.

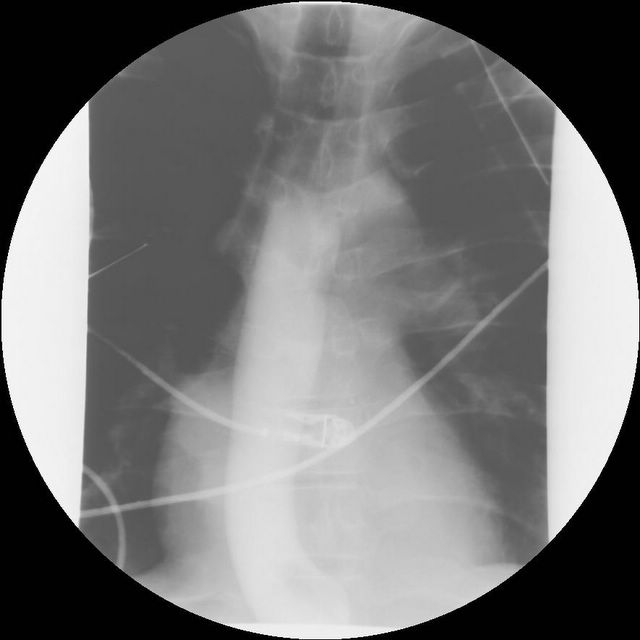
The black line points to fragments anterior to the verterbral body. That is the bullet went in between the aorta and the verterbra. And this patient was real skinny, not a great deal of fat back there. Here is the AP view:
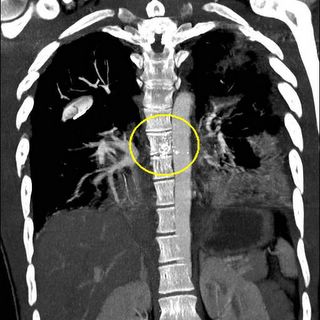
Really close there. So his aorta was OK. No air leak in his chest tubes and the path was too posterior to affect the airway. Next thing was the esophagus:

O.K. by barium swallow. But the CT of his abdomen also showed:


A injury to his liver. So the bullet had to penetrate the diaphragm at least once. Here are some images from the reconstruction:
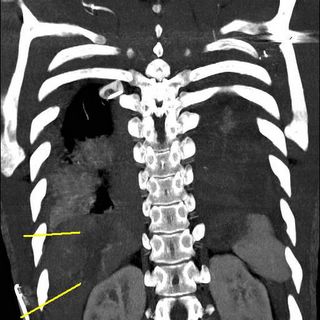

Showing the tract of the projectile. The patient was still tachycardic but responding to fluids. Off to the OR.
The injury was difficult to expose due to its' location. The diaphragm injury was within the boundaries of the right triangular ligament through the "bare area" of the liver. The difficulty of exposure is one reason the treatment of retrohepatic venous injuries is so difficult. It was small, about the size of a .22 caliber projectile. A portal branch was ligated with a clip and the diffuse oozing was controlled with fibrin glue. Commercial hemostatic agents are available but the largest volume is 5cc. I make my own with cryoprecipitate, thrombin, and calcium. I can usually get 180 cc at least of glue. He required 2 units of blood. Anesthesia did a good job of keeping him warm and he actually went from 96.4 degrees to 98 degrees.
Transmediastinal wounds are difficult to take care of because of the multimodality apprach required. Patients that are hemodynamically unstable must be taken promptly to the OR. The rest must have their vascular and aerodigestive structures evaluated.
The gold standard used to be arch aortogram, bronchoscopy, and barium swallow. The advent of multi-slice CT scanning has largely reduced the use of the first two modalities, being reserved for inconclusive studies. Barium swallow still has its' role.
Just a few millimeters between life and death.....
Sometimes millimeters make the difference. 20-ish year old shot in the right side of his back. He was tachycardic at the referring facility, but otherwise stable. No chest tubes were placed. Here is his initial CXR:
Interestingly the left pneumothorax and the bullet in the left side of his chest was not mentioned during the presentation. A better view (with some chest tubes) can be seen in the scout film of his CT:
A paperclip marks the entry wound. Lots of vital things live between point "A" and point "B". Since he was hemodynamically stable he could undergo a complete radiographic evaluation instead of an exploration. After discussion with the radiologist he underwent a CT angiogram of his chest rather than a conventional angiogram:
This is one of the leftmost slices of the reconstruction showing the projectile posterior to the left scapula.

The black line points to fragments anterior to the verterbral body. That is the bullet went in between the aorta and the verterbra. And this patient was real skinny, not a great deal of fat back there. Here is the AP view:

Really close there. So his aorta was OK. No air leak in his chest tubes and the path was too posterior to affect the airway. Next thing was the esophagus:
O.K. by barium swallow. But the CT of his abdomen also showed:


A injury to his liver. So the bullet had to penetrate the diaphragm at least once. Here are some images from the reconstruction:


Showing the tract of the projectile. The patient was still tachycardic but responding to fluids. Off to the OR.
The injury was difficult to expose due to its' location. The diaphragm injury was within the boundaries of the right triangular ligament through the "bare area" of the liver. The difficulty of exposure is one reason the treatment of retrohepatic venous injuries is so difficult. It was small, about the size of a .22 caliber projectile. A portal branch was ligated with a clip and the diffuse oozing was controlled with fibrin glue. Commercial hemostatic agents are available but the largest volume is 5cc. I make my own with cryoprecipitate, thrombin, and calcium. I can usually get 180 cc at least of glue. He required 2 units of blood. Anesthesia did a good job of keeping him warm and he actually went from 96.4 degrees to 98 degrees.
Transmediastinal wounds are difficult to take care of because of the multimodality apprach required. Patients that are hemodynamically unstable must be taken promptly to the OR. The rest must have their vascular and aerodigestive structures evaluated.
The gold standard used to be arch aortogram, bronchoscopy, and barium swallow. The advent of multi-slice CT scanning has largely reduced the use of the first two modalities, being reserved for inconclusive studies. Barium swallow still has its' role.
Just a few millimeters between life and death.....
Labels: Tales from the Trauma Service
|![]()





