Thursday, May 19, 2005
Tales From the Trauma Service XI ......
A husband and wife, t-boned on the wife's side of the vehicle. She complains of abdominal pain and is hypotensive. She does not respond to fluids or transfused blood. She has a minor pelvic fracture and some free fluid on FAST. Off to the OR...
About 2000cc of blood within the peritoneum. Spleen, large and small bowel, and stomach all OK. A small hematoma surrounding the pelvic fracture. The edge of the right lobe of the liver was pendulous. The dome of the liver was without injury. Inspection of the posterior segment demonstrates a large laceration extending into the porto-caval region.
This is when the wheels begin to come off.
At this time the patient develops EKG changes and bradycardia. I pack the injury off and occlude the aorta. After some CPR, defib, and drugs we regain a pulse and an adequate BP. Her PT was 20 when we hit the room and now her temp is 92 degrees. I repack the RUQ and close her with a VAC. She arrests again before we can get her to the ICU, but again drugs and CPR do the trick. Up to the unit where she codes again and despite 30 minutes of ACLS magic, she expires.
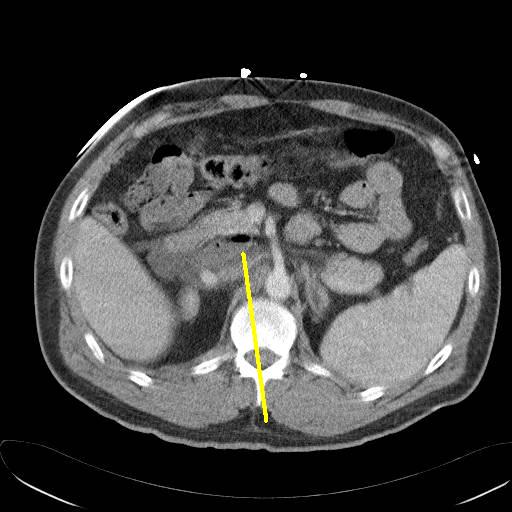
In the meantime, her husband is undergoing his evaluation. And the stab wound to the chest that came in before these two still needs a chest tube. The husband is hemodynamicaly stable and complains of right flank and back pain. The CT of the husband's abdomen:
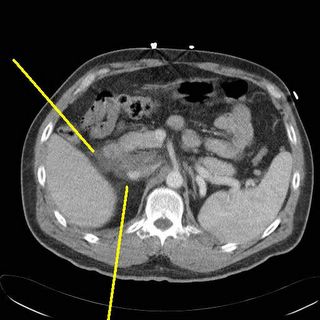
Some duodenal thickening and periduodenal fluid (yellow).

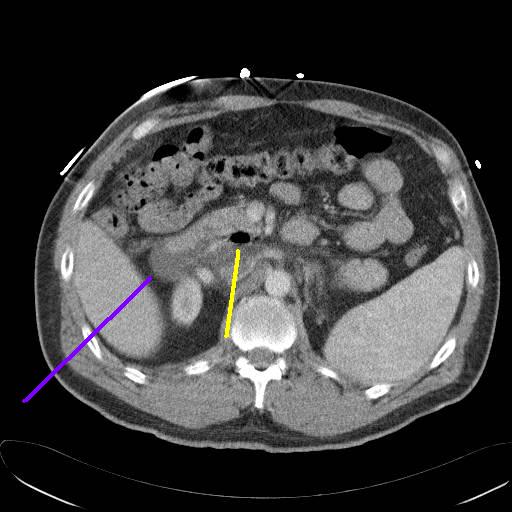
Uh-oh, is that free air I see? (yellow again)
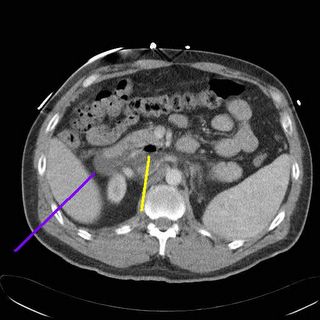
Another image, fluid at the blue line, air at the yellow.
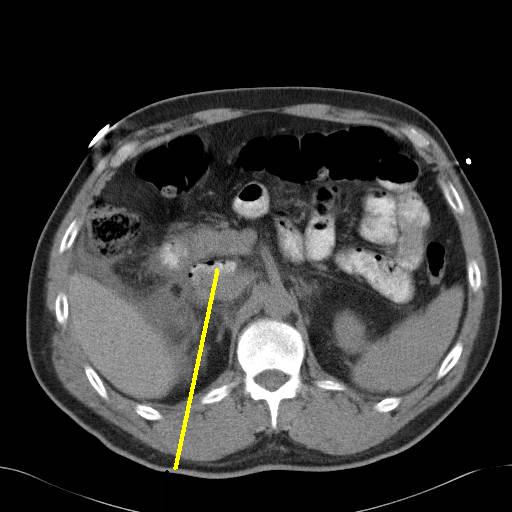
The radiologist recommended that the study could be repeated in a few days. I don't thinks so. I repeat it a few hours later with oral contrast:
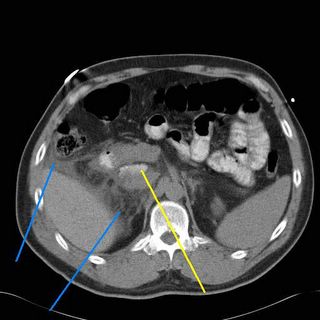
More fluid seen at the blue lines and contrast within the area that held free air earlier.
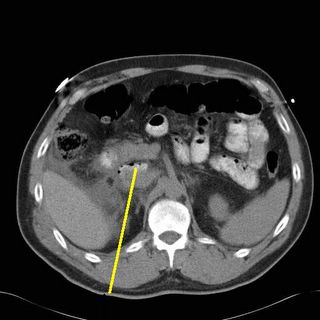
Air and contrast at the yellow area. SO a duodenal injury cannot be ruled out. Duodenal injuries are troublesome because they are difficult to diagnose, can be devastating if undiagnosed promptly, and it is an unforgiving organ to repair. The mortality and morbidity increase almost twofold if diagnosis is delayed over 24 hours. Surgical wisdom tells us that the reason God put the duodenum and pancreas posteriorly is that so surgeons wouldn't mess with it. So off I go on a journey through God's country.
Upon opening a fair amount of turbid fluid was seen. A right-sided medial visceral rotation was performed. The abdomen was explored and no other injury was found. The duodenum was Kocherized (rotated to the left) and what do I find?

Sorry it's blurry. Black line is the IVC, light blue lines are the duodenum, green line the posterior surface of the pancreas, and the dark blue line a duodenal diverticulum, which was the site of the rupture. Yahoo. Now what to do about repair? Fortunately the injury itself was able to be repaired primarily, but the trick is what to do to protect the repair long enough for it to heal. Obviously a closed-suction drain was placed. I opted for pyloric exclusion and gastrojejunostomy. The pylorus was sewn shut with a heavy PDS and a Billroth II-type gastrojejunostomy was performed. A feeding jejunostomy was also inserted. Here is a diagram:
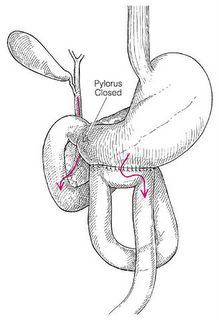
The idea is that the pylorus will remain closed long enough for the repair to heal. This sort of operation takes time and in an unstable patient who is cold and coagulopathic time is a luxury you may not have. In that case damage control with repair and wide drainage is your primary move. He is doing fine so far.
A husband and wife, t-boned on the wife's side of the vehicle. She complains of abdominal pain and is hypotensive. She does not respond to fluids or transfused blood. She has a minor pelvic fracture and some free fluid on FAST. Off to the OR...
About 2000cc of blood within the peritoneum. Spleen, large and small bowel, and stomach all OK. A small hematoma surrounding the pelvic fracture. The edge of the right lobe of the liver was pendulous. The dome of the liver was without injury. Inspection of the posterior segment demonstrates a large laceration extending into the porto-caval region.
This is when the wheels begin to come off.
At this time the patient develops EKG changes and bradycardia. I pack the injury off and occlude the aorta. After some CPR, defib, and drugs we regain a pulse and an adequate BP. Her PT was 20 when we hit the room and now her temp is 92 degrees. I repack the RUQ and close her with a VAC. She arrests again before we can get her to the ICU, but again drugs and CPR do the trick. Up to the unit where she codes again and despite 30 minutes of ACLS magic, she expires.
In the meantime, her husband is undergoing his evaluation. And the stab wound to the chest that came in before these two still needs a chest tube. The husband is hemodynamicaly stable and complains of right flank and back pain. The CT of the husband's abdomen:

Some duodenal thickening and periduodenal fluid (yellow).
Uh-oh, is that free air I see? (yellow again)
Another image, fluid at the blue line, air at the yellow.
The radiologist recommended that the study could be repeated in a few days. I don't thinks so. I repeat it a few hours later with oral contrast:

More fluid seen at the blue lines and contrast within the area that held free air earlier.
Air and contrast at the yellow area. SO a duodenal injury cannot be ruled out. Duodenal injuries are troublesome because they are difficult to diagnose, can be devastating if undiagnosed promptly, and it is an unforgiving organ to repair. The mortality and morbidity increase almost twofold if diagnosis is delayed over 24 hours. Surgical wisdom tells us that the reason God put the duodenum and pancreas posteriorly is that so surgeons wouldn't mess with it. So off I go on a journey through God's country.
Upon opening a fair amount of turbid fluid was seen. A right-sided medial visceral rotation was performed. The abdomen was explored and no other injury was found. The duodenum was Kocherized (rotated to the left) and what do I find?

Sorry it's blurry. Black line is the IVC, light blue lines are the duodenum, green line the posterior surface of the pancreas, and the dark blue line a duodenal diverticulum, which was the site of the rupture. Yahoo. Now what to do about repair? Fortunately the injury itself was able to be repaired primarily, but the trick is what to do to protect the repair long enough for it to heal. Obviously a closed-suction drain was placed. I opted for pyloric exclusion and gastrojejunostomy. The pylorus was sewn shut with a heavy PDS and a Billroth II-type gastrojejunostomy was performed. A feeding jejunostomy was also inserted. Here is a diagram:

The idea is that the pylorus will remain closed long enough for the repair to heal. This sort of operation takes time and in an unstable patient who is cold and coagulopathic time is a luxury you may not have. In that case damage control with repair and wide drainage is your primary move. He is doing fine so far.
Labels: Tales from the Trauma Service
|![]()





