Monday, September 13, 2004
Where Did It Go??????
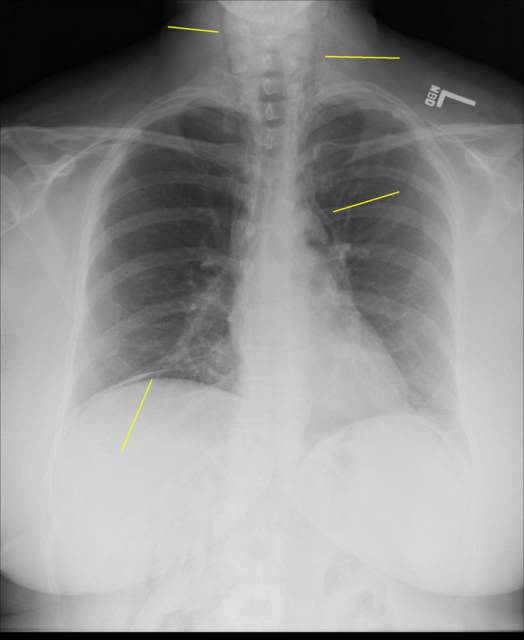
Tales from the OR continues....50-ish year old woman with a history of diverticular perforation in the past which required a 3-stage procedure (drainage/diversion, resection, and finally colostomy takedown) to resolve about 3 years ago. Had symptoms c/w ulcerative colitis and underwent uneventful colostomy and biopsy. About 8 hours post-procedure she began to c/o chest and neck pain. Went to the ED and obtained the following CXR:

The yellow lines point to air in unusual places. I wasn't entirely convinced that the air along the right diaphragm was intraperitoneal as you could not see the line of the right hemidiaphragm all the way to the midline. Obtained a CT scan:

Which shows both intraperitoneal and retroperitoneal air.

The amount of air is such that the kidney is outlined.

There is a hernia at the old stoma site. The air in the mesentery appears here. The preop diagnosis was a colonic perforation due to the colonoscopy. The treatment for this is exploration and primary repair. Primary repair is possible due to the prepared colon after a colonoscopy.
Upon entering the abdomen there was not the usual audible rush of air that comes with entry into the peritoneum. An extensive adhesiolysis followed and I was fortunate not to create an enterotomy. Given the preponderance of the air on the right side my efforts were concentrated there. There was a good deal of air within the wall of the colon and mesentery. No spillage, gross perforation, or colonic ischemia was seen. The colon was defatted extensively. This was approached gingerly since if a hole was discovered, the question could come up was it there, or did I create it? After all this I had three options: blind resection, close up and go home, or provocative testing. Given the late hour the tests I could perform were limited. Here's what I did.
Bowel clamps were placed on the terminal ileum and distal transverse colon. The colon was cannulated with a 16-gauge angiocath and about 400cc of air was insufflated. This achieved a distention similar to that of colonoscopy. The colon was submerged under saline and observed for bubbles. None seen. Given the possibility of a perforation into the mesentery that air may not reveal, I then instilled about 250cc of methylene blue solution. No blue anywhere. Did the same thing to the left side of the colon, no spillage. Gave it several looks during closure, still no blue. There was not only frustration that no perforation was found, but a concern that I was missing something.
There is a level of comfort in the practice of medicine and surgery that can be roughly described as the "sleep of the just". I think you know what I mean. Cases like this do little to help my sleep. But I thought that a blind resection was too radical, that any clinically significant perforation would have been identified. I closed and went to bed.
She is doing well. Postop CXR shows resolution of the free air. |
Tales from the OR continues....50-ish year old woman with a history of diverticular perforation in the past which required a 3-stage procedure (drainage/diversion, resection, and finally colostomy takedown) to resolve about 3 years ago. Had symptoms c/w ulcerative colitis and underwent uneventful colostomy and biopsy. About 8 hours post-procedure she began to c/o chest and neck pain. Went to the ED and obtained the following CXR:
The yellow lines point to air in unusual places. I wasn't entirely convinced that the air along the right diaphragm was intraperitoneal as you could not see the line of the right hemidiaphragm all the way to the midline. Obtained a CT scan:

Which shows both intraperitoneal and retroperitoneal air.

The amount of air is such that the kidney is outlined.

There is a hernia at the old stoma site. The air in the mesentery appears here. The preop diagnosis was a colonic perforation due to the colonoscopy. The treatment for this is exploration and primary repair. Primary repair is possible due to the prepared colon after a colonoscopy.
Upon entering the abdomen there was not the usual audible rush of air that comes with entry into the peritoneum. An extensive adhesiolysis followed and I was fortunate not to create an enterotomy. Given the preponderance of the air on the right side my efforts were concentrated there. There was a good deal of air within the wall of the colon and mesentery. No spillage, gross perforation, or colonic ischemia was seen. The colon was defatted extensively. This was approached gingerly since if a hole was discovered, the question could come up was it there, or did I create it? After all this I had three options: blind resection, close up and go home, or provocative testing. Given the late hour the tests I could perform were limited. Here's what I did.
Bowel clamps were placed on the terminal ileum and distal transverse colon. The colon was cannulated with a 16-gauge angiocath and about 400cc of air was insufflated. This achieved a distention similar to that of colonoscopy. The colon was submerged under saline and observed for bubbles. None seen. Given the possibility of a perforation into the mesentery that air may not reveal, I then instilled about 250cc of methylene blue solution. No blue anywhere. Did the same thing to the left side of the colon, no spillage. Gave it several looks during closure, still no blue. There was not only frustration that no perforation was found, but a concern that I was missing something.
There is a level of comfort in the practice of medicine and surgery that can be roughly described as the "sleep of the just". I think you know what I mean. Cases like this do little to help my sleep. But I thought that a blind resection was too radical, that any clinically significant perforation would have been identified. I closed and went to bed.
She is doing well. Postop CXR shows resolution of the free air. |
![]()





