Wednesday, June 01, 2005
Tales from the Operating Room VI....
Or: "How the Simple Things Can be a Challenge"
A teenager in remission from lymphoma. The infusaport has been in place for over a year and has not been accessed in over 4 months. It was placed at another facility via a left subclavian approach. The local pediatrician who had assumed care sent the patient to me for removal.
All was going well. I cut down on the "button", dissected it out, and removed the catheter. No resistance was met. Imagine my surprise when I examined the specimen:

That looks a little short to me. Brought in the C-arm and looky here:
Proximal and distal ends marked. Since the preferred approach is now endovascular I closed the wound. Here is a CXR obtained before going to the angio suite:

Ends again marked. Some images from the endovascular attempt:
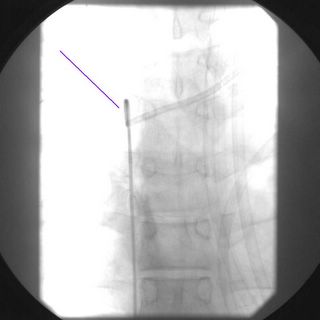
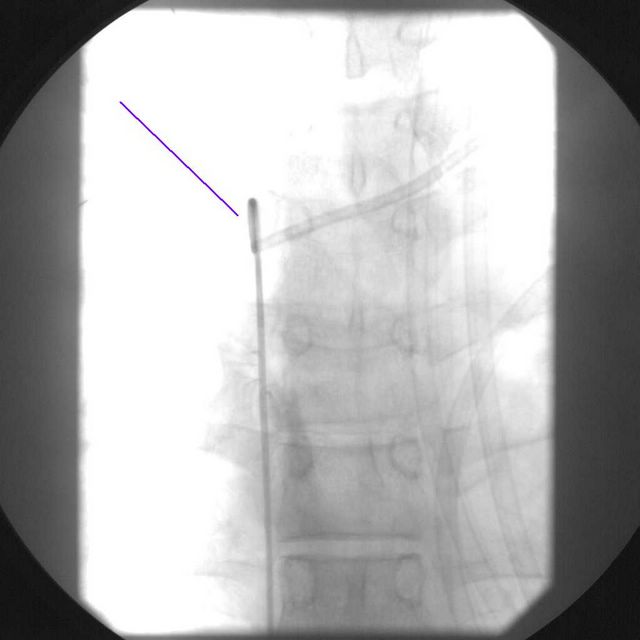
A catheter from a femoral approach. Multiple attempts were made with a snare to grab the distal end.
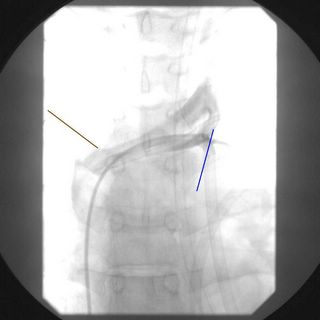
Attempts made to grab proximally. Contrast from a venogram can be seen. The radiologist estimates that about 1-2 cm of the catheter is extraluminal. The catheter seems to be held in place by a fibrin sheath. I review the images with a thoracic surgery colleague who felt that a cutdown approach to retrieve it would be possible. With by thoracic surgeon as a backup off we go.
Using c-arm I localize the catheter and cut down on it. Split the pectoralis major. Cell layer by cell layer divided with frequent re-checks of the flouroscopy to make sure it does not migrate. Eventually I found it and out it comes:

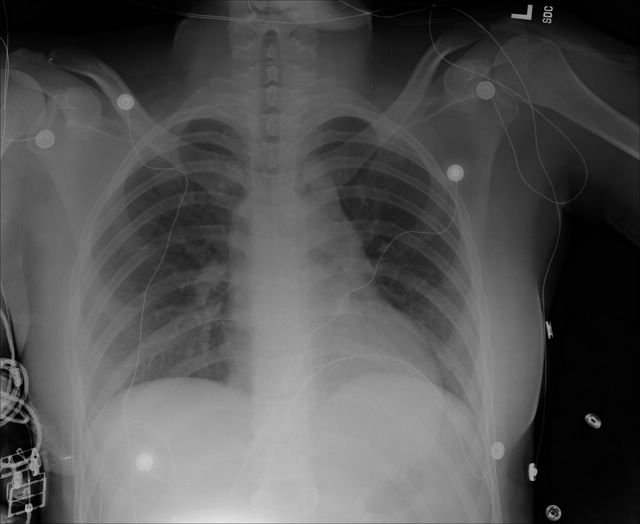
The postop CXR:

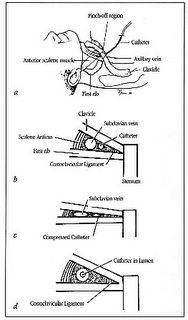
How did this happen? A phenomenon known as "Pinch off Syndrome" has been described with subclavian catheters. It has to do with the anatomy of the space between the clavicle and first rib, as seen here:
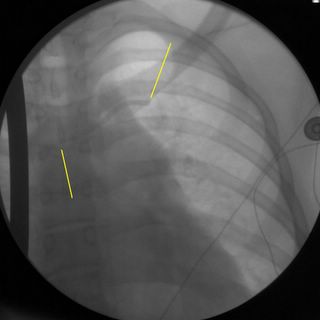
The particular placement of this catheter also contributed:
(You may need to zoom in). The top yellow line represents the superior curve and the lower yellow line represents where the catheter enters the costoclavicular space at almost a right angle. The catheter portions were crimped at that site. The catheter had probably been divided for a while. Yet another reason that I do not like subclavian placement of long-term catheters |
Or: "How the Simple Things Can be a Challenge"
A teenager in remission from lymphoma. The infusaport has been in place for over a year and has not been accessed in over 4 months. It was placed at another facility via a left subclavian approach. The local pediatrician who had assumed care sent the patient to me for removal.
All was going well. I cut down on the "button", dissected it out, and removed the catheter. No resistance was met. Imagine my surprise when I examined the specimen:

That looks a little short to me. Brought in the C-arm and looky here:

Proximal and distal ends marked. Since the preferred approach is now endovascular I closed the wound. Here is a CXR obtained before going to the angio suite:

Ends again marked. Some images from the endovascular attempt:
A catheter from a femoral approach. Multiple attempts were made with a snare to grab the distal end.

Attempts made to grab proximally. Contrast from a venogram can be seen. The radiologist estimates that about 1-2 cm of the catheter is extraluminal. The catheter seems to be held in place by a fibrin sheath. I review the images with a thoracic surgery colleague who felt that a cutdown approach to retrieve it would be possible. With by thoracic surgeon as a backup off we go.
Using c-arm I localize the catheter and cut down on it. Split the pectoralis major. Cell layer by cell layer divided with frequent re-checks of the flouroscopy to make sure it does not migrate. Eventually I found it and out it comes:

The postop CXR:
How did this happen? A phenomenon known as "Pinch off Syndrome" has been described with subclavian catheters. It has to do with the anatomy of the space between the clavicle and first rib, as seen here:
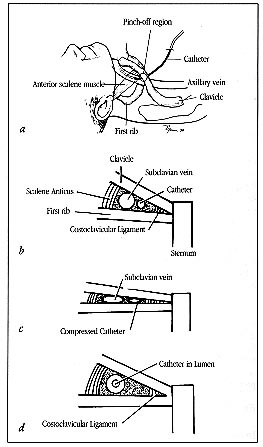
The costoclavicular space. Anatomic (a) and diagrammatic (b) representations. If the catheter passes through the areolar tissue of this space outside the vessel lumen (a medical insertion), it is vulnerable to compression by the clavicle and first rib. (c) Repeated compressive and shearing forces act on the catheter as the shoulder is raised and lowered. (d) A more lateral insertion of the catheter allows it to travel within the subclavian vein. This vessel lies in a more capacious region, and thus by geometric considerations it is protected from compression.
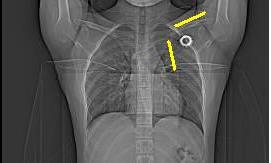
The particular placement of this catheter also contributed:

(You may need to zoom in). The top yellow line represents the superior curve and the lower yellow line represents where the catheter enters the costoclavicular space at almost a right angle. The catheter portions were crimped at that site. The catheter had probably been divided for a while. Yet another reason that I do not like subclavian placement of long-term catheters |
![]()





