Monday, January 08, 2007
The Upcoming CON Battle.....
The Georgia General Assembly kicks off today and tort refrom is not the only health-related subject that is up for debate this year. I saw this post from Peach Pundit about the upcoming battle over Certificate of Need (CON) in Georgia a few weks ago and was moved to comment, given the impact that CON will have this year.
For those unfamiliar, a CON is a permit that hospitals and other healthcare institutions must aquire before construction of facilities (even non-medical ones, such as a parking deck) or offer a new service (such as cardiac surgery).
The rationale from the State of Georgia's .Certificate of Need Frequently Asked Questions Review Guide:
There are some projects that are exempt from the CON process:
What has brought this to the forefront was our old friend Dr. Bagnato. Word around the campfire became that Dr. Bagnato's suggested motivation for his lawsuit was Pheobe Putney's opposition to his CON for an ambulatory surgery center. The wrinkle here is that in the state of Georgia general surgery is not considered a single specialty so Dr. Bagnato was not allowed to avoid the CON process.
Dr. Bagnato has found a voice in the Georgia Society of General Surgeons, a group that has been fighting to change the CON laws since its' inception. (Full disclosure, I am not a menber) While I can understand their frustration I do not agree with their reasoning or the protrayal of hospitals.
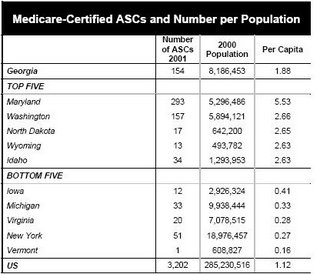
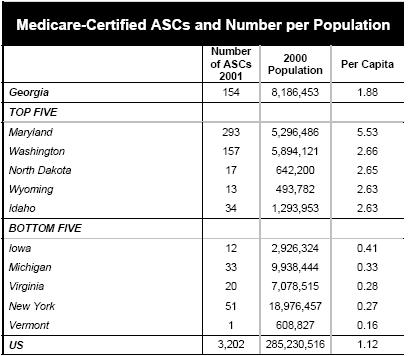
I will be the first to admit my take is skewed by my role in the trauma program in River City, so caveat empetor. I have seen plastic surgeons, ortopedic surgeons, urologists and otolaryngologists stop taking trauma and emergency call because they can do the vast majority of their procedures in office or an ambulatory surgery center (ASC) and not rely on the hospital. EMTALA also places a burden on hospitals (and physicians) that are not shared by the ASC or office-based surgery suites. And despite what may be said, medicine in 2007 is not a free-market system, and the usual rules of supply and demand do not apply. There is some irony that the GSGS supports a statewide trauma network, but is making it more difficult to obtain the coverage needed to make it work (as does the Medical Association of Georgia). We certainly don't lack for ASC's in Georgia as this chart shows we have above the national average per captia number of ASC's:
But the reccommendations are out. For those who wish to read the entire 267 pages of the report, here you go. But for the easily bored, here are the reccommendations from the executive summary that pertain to general surgery and ASC's:
My physician colleagues need to tread carefully here. The hospitals can make a very persuasive argument aimed at the public concerning lack of access to care. If left to their own devices I doubt many of these ASC's will take care of the medically complex or the underinsured. It will be an interesting battle.
The Georgia General Assembly kicks off today and tort refrom is not the only health-related subject that is up for debate this year. I saw this post from Peach Pundit about the upcoming battle over Certificate of Need (CON) in Georgia a few weks ago and was moved to comment, given the impact that CON will have this year.
For those unfamiliar, a CON is a permit that hospitals and other healthcare institutions must aquire before construction of facilities (even non-medical ones, such as a parking deck) or offer a new service (such as cardiac surgery).
The rationale from the State of Georgia's .Certificate of Need Frequently Asked Questions Review Guide:
Georgia’s Certificate of Need Program was codified by the Georgia legislature in 1979 in Georgia's Health Planning Statute, Title 31, Chapter 6. The purpose of the CON program is to insure the availability of adequate health care services to meet the need of all Georgians, while safeguarding against the unnecessary duplication of services that perpetuate the costs of healthcare services. The Department of Community Health was created in 1999 and the administration of the CON Program was placed within the Department.
There are some projects that are exempt from the CON process:
An Ambulatory Surgery Facility that is physician owned, office-based, and single-specialty, the establishment and development of which does not exceed the limited-purpose physician-owned ambulatory surgery centers threshold.According to the footnote the 2004 figure was $1,436,356. The key term above is "single specialty", a term that has generated some controversey.
What has brought this to the forefront was our old friend Dr. Bagnato. Word around the campfire became that Dr. Bagnato's suggested motivation for his lawsuit was Pheobe Putney's opposition to his CON for an ambulatory surgery center. The wrinkle here is that in the state of Georgia general surgery is not considered a single specialty so Dr. Bagnato was not allowed to avoid the CON process.
Dr. Bagnato has found a voice in the Georgia Society of General Surgeons, a group that has been fighting to change the CON laws since its' inception. (Full disclosure, I am not a menber) While I can understand their frustration I do not agree with their reasoning or the protrayal of hospitals.
I will be the first to admit my take is skewed by my role in the trauma program in River City, so caveat empetor. I have seen plastic surgeons, ortopedic surgeons, urologists and otolaryngologists stop taking trauma and emergency call because they can do the vast majority of their procedures in office or an ambulatory surgery center (ASC) and not rely on the hospital. EMTALA also places a burden on hospitals (and physicians) that are not shared by the ASC or office-based surgery suites. And despite what may be said, medicine in 2007 is not a free-market system, and the usual rules of supply and demand do not apply. There is some irony that the GSGS supports a statewide trauma network, but is making it more difficult to obtain the coverage needed to make it work (as does the Medical Association of Georgia). We certainly don't lack for ASC's in Georgia as this chart shows we have above the national average per captia number of ASC's:
But the reccommendations are out. For those who wish to read the entire 267 pages of the report, here you go. But for the easily bored, here are the reccommendations from the executive summary that pertain to general surgery and ASC's:
Recommendation 14.1 (5 Agree, 1 Disagrees, 4 AbstainOn this Dr. Bagnato and I agree. Treat us the same as our orthopedic, urologic, and otolayngologic peers.
Treat General Surgery in a consistent manner as all other single specialties.)
The majority of the Commission recommends that General Surgery be treated in a manner consistent with all other singe specialties, regardless of the regulatory requirement for single specialty facilities.
One member disagrees and maintains that general surgery should be treated as a multi-specialty because of the complex nature of the cases that a general surgeon may perform.
Recommendation 14.2 (5 Agree, 3 Disagree, 2 Abstain)This would allow for ASC's to be built on every street corner if so desired, since need criteria would not be factored into a CON decision. Physicians who utilize an ASC would be required to maintain hospital staff priveledges and take ED call. Another objection, in addition to those described above, is that this would allow hospitals an unfair advantage since if a physician were to resign or be removed from staff, theit CON could be affected. Then there is an absolutist position:
Abolish entirely the exemption for freestanding single specialty, office-based, physician-owned ambulatory surgery centers and require physician-owned limited purpose ambulatory surgery centers to obtain a Certificate from the Department. Upon application, such applicants would not be required to address need criteria but would be required to make indigent and charity care commitments, to accept Medicaid, to supply data to the Department of Community Health, and to verify that all its physicians are members of a hospital staff and are willing to accept emergency room coverage.
The membership of the Commission was sharply divided on the issue of physician-owned single specialty ambulatory surgery centers, which are currently exempt from Certificate of Need if the center can be established for a dollar amount less than approximately $1.6 million. One contingent of the Commission agrees with the recommendation that the current exemption be abolished and that limited-purpose, physician- owned ambulatory surgery centers (“ASC”) obtain a Certificate, although such centers would be free from an objective need methodology. Such ASCs would be required to commit to the provision of indigent and charity care at a level of 3 percent of adjusted gross revenues. In addition, this contingent recommends that these ASCs agree to accept Medicaid, if at all possible, and provide services as a minimum community standard, that such facilities agree to provide annual data to the Department, and that all physicians who perform procedures at the facility be required to hold hospital staff privileges, if possible, and to accept ER coverage. The members who agree with this recommendation do so because freestanding single-specialty ambulatory surgery centers have been shown to be high quality and low cost alternatives. These members who argue for less regulatory control contend that to artificially restrain these services raises costs reduces efficiency, and prevents physicians from billing facility fees.
Other members disagreed with this recommendation and maintain that the exemption for physician-owned ambulatory surgery centers should be abolished and that such centers should be required to obtain a Certificate of Need addressing all applicable review criteria including a determination of need. These members are concerned that if ambulatory surgery centers are allowed to proliferate significantly, hospitals will not have a financially sustainable business model. Mainly, these members maintain that ambulatory surgery centers take low acuity, paying patients, and leave hospitals to treat the complex cases and individuals without the ability to pay.
The CON Commission has been unable to reach consensus with regard to the best policy to address this difficult issue because its root causes involve complex factors relating to reimbursement and costs that are beyond the CON program’s purview. A real and sustainable solution to this dilemma will require a health policy approach that corrects the cost and payment problems for both professional services and hospital-based services, particularly with respect to the under-insured and uninsured.
Recommendation 14.3 (3 Agree, 3 Disagree, 4 Abstain)As an aside, what's with the abstentions? the Chair and vice-chair and another member (Dr. Meadows) were ex officio members of the committee (probably due to their being state employees) but the report states that on the ASC subject they did vote. The report makes no mention of how each member voted or why those that abstained did so (I have this information but cannot confirm it). Given the high stakes involved I believe that some weaseled out of making a commitment. A few other reccommendations of note that do not relate to surgery, but may have a higher impact:
Abolish the exemption for physician-owned, office-based, single specialty ambulatory surgery centers and require such facilities to obtain a Certificate of Need under the exact same standards as all other ambulatory surgery centers.
The original recommendation of the Specialized Services Sub-Committee was to abolish the current ASC exemption and require all ASCs to obtain a Certificate of Need without exception. The full Commission discussed this recommendation, but was sharply divided and no final conclusion was reached on the recommendation.
and....
Recommendation 6.0 (4 Agree, 1 Disagrees, 5 Abstain)
Deregulate diagnostic cardiac catheterization and require therapeutic catheterizations to be performed only by providers approved to offer open heart surgery.
The members of the Commission who support the deregulation of adult diagnostic cardiac catheterization maintain that deregulating diagnostic cardiac catheterization will allow for the proliferation of these services in the market assuring access to residents in all areas of the state. Such members feel that this service is a valuable service to the citizens of the state and has been shown to save lives, particularly in states such as Georgia with high rates of coronary disease. These members feel that the regulation of the quality of this service could be managed by Licensure.
One member of the Commission disagrees. This member feels that this service should continue to be regulated by Certificate of Need. Because cardiac catheterization is such a specialized service, certain quality standards must be met to achieve the best possible outcomes. Because the American College of Cardiology recommends that minimum volumes be maintained to ensure the quality of the service, this member feels the Certificate of Need process ensures that there will not be a proliferation of low volume providers who won’t maintain the same quality as high volume providers.
Several members of the Commission report that this recommendation should only apply to hospital-based cardiac catheterization and not to freestanding cath programs.
Recommendation 7.0 (6 Agree, 1 Disagrees, 3 Abstain)The hospitals are already planning their next move:
Deregulate Level I perinatal services and continue regulation of Level II and Neonatal Intensive Care.
Most members of the Commission recommend that Level I perinatal services be deregulated because these services are already provided by most hospitals in the state and do not require specialized labor. These members believe that access to perinatal and obstetrical care will be enhanced by their recommendation. The fact that federal law already requires a facility to treat a woman in active labor further supports this recommendation. The members who make this recommendation maintain that Level II and Level III services should continue to be regulated by CON because of the highly- skilled nature of these services and the workforce that is required to support them. One member of this group further believed that Level II should be deregulated in addition to Level I.
One member of the Commission made the recommendation to maintain existing CON regulation for this service. This member believes that maintaining Certificate of Need regulation of Level I perinatal services will address the problem of large fixed costs incurred by facilities that provide these services and the shortage of skilled workforce.
Several members of the Commission report that this recommendation should be limited to Level 1 perinatal services at hospitals and should not be construed as a recommendation regarding freestanding facilities.
Concerned about a possible hit to their bottom line, metro Atlanta hospitals are preparing to put a few newly proposed state health-care regulations under the knife.
.....Hospitals argue that physician-owned surgery centers siphon off their best-paying patients, leaving the burden of the uninsured for hospitals to bear.
Recent financial data just released by the state Department of Community Health, which tracks the performance of hospitals each year, shows that metro Atlanta's 25 largest hospitals spent nearly $485 million combined on uncompensated, indigent and charity care in 2005. That's up 12 percent from $435 million in 2004.
The recommendation "is just one more knife in the hospitals' back, and it's a big knife," said Michael Rovinsky, president of the health-care consulting firm Integrity Consulting Group. "General surgery accounts for a lot of profitable procedures. This is the one [recommendation] that's going to be fought the hardest."
....But the proposal to classify general surgery as a single specialty could be damaging to many hospitals, especially as they continue to fight rising costs to care for the poor and uninsured.
"It would have a financial impact," said Holly Snow, Piedmont's vice president of government and external affairs.
The commission anticipated the controversy, and in its recommendations says all outpatient surgery centers must commit to serving the indigent and uninsured.
Other possibly contentious recommendations are also included in the commission report. One permits hospitals wanting to launch general labor and delivery programs to circumvent the certificate-of-need process. The same goes for hospitals trying to start up diagnostic heart catheterization programs. The catheterization procedure involves a thin, hollow tube that is threaded through the body to examine the heart's chambers.
My physician colleagues need to tread carefully here. The hospitals can make a very persuasive argument aimed at the public concerning lack of access to care. If left to their own devices I doubt many of these ASC's will take care of the medically complex or the underinsured. It will be an interesting battle.
Labels: Georgia
|![]()





