Tuesday, February 28, 2006
Grand Rounds Vol II No. 23......
Welcome to Grand Rounds, the weekly roundup of the medical blogosphere. This week's tour is accompanied by the artwork of surgeon/painter Joseph Wilder. Enjoy!!
Removing Gloves
The Patient Encounter as Literary Exposition:
The Cheerful Oncologist combines his own flair with the lyrics of Lennon/McCartney in discussing withdrawal of chemotherapy.
While Dr. Wilder is best known for painting sports and surgery, Maria writes of a patient who paints something else.
Dr. Charles has a brush with greatness, but humbly passes on it.
Sunlight Follows Me shares the story of a man finding peace and comfort in the arms of God.
Doc Shazam tells of the signing out and bad news.

Five Surgeons
The Casualties of Substance Abuse:
Rita Schwab posts about an increasingly common problem, dealing with the impaired physician.
Keith Carlson is able to find compassion in his heart as he treats the members of his "poor, chronically ill and generally disenfranchised community".

Surgeons as Heroes
Fun with My Colleagues:
keagirl plays the old "don't ask, don't tell"game with the always entertaining "foreign body" patient.
As part of his "Tales of the Trauma Service" Orac really develops a taste for his work. Didn't anyone tell him those things were dangerous? Too bad no pictures.
Of course when the likes of me get around a patient things can and do go wrong, as Geena points out.
The Grunt Doc rages against the machine and their increasingly specialized CME requirements. Come take my ATLS course Allen, it will be worth your while.
Scrubbing Hands
Point/Counterpoint:
Insureblog thinks Health Savings Accounts are the way to control health costs.
Jill Quadagno however,disagrees.
Neonatal Doc looks at the complex issue of giving or withholding care to sick children.

The Preoperative Examination
The Patients that Challenge Us:
The Blog That Ate Manhattan posts about a pregnant recipient of the "gift that keeps on giving".
Big Mama lets us know of a family's disappointment that she is a real doctor and doesn't play one on TV.
Dr. Emer writes about the problems of the patient with chronic pain.

Gowned and Gloved
Medicine and Socioeconomics:
Will Hotels.com make a commercial with ambulances rushing to the hotel rather than black Suburbans? Kevin relays the story of Canadian tourist medicine. Will the "Roaming Gnome" now appear in a white coat?
Fellow Aggravated Surgeon delivers a dissetation on the high sums that the new math can generate.
Hospital Impact looks at the three types of hospital administrators the good, the bad, and the ugly.
Health Business Blog examines a formula controversy in Boston.
Dr. Crippen issues a challenge to those physicians who support the death penalty.
Dr. Newberry pines for the good old days.

Concentration in Surgery
The Bugs Among Us:
Dr. Smith gives us the latest on the bug that ate Boulder.
Interested Participant comments on the growing problem of community MRSA.

Contemplation before Surgery
Research Corner:
Dr. Ng asks the common post-steak dinner question: Why does asparagus make my pee stink?
The Abel Pharmboy examines the pharmacological impact of a recent Supreme Court decision.
With training can you snatch the pebble from the Master's hand? Always Learning lets us know that functional MRI shows it happening.

Sharp Dissection
Kids do the Darndest Things....
And as the Geek Nurse shows we can do the darnest things to them.
Dr. Andy agrees with compulsory vaccination, with some execptions.
My grasp extends far beyond my inbox. Thus arrives
Flea with his meningitis gamble.
Do you still feed a fever? Emergiblog fills us in.
Dr. Hebert recognizes that resistance is futile where TV and kids are concerned.
Threading the Needle
Last but not least:
A woman with many hats is full of the Olympic spirit as are the athletes overcoming medical difficulties.
The Insider fills us in on another drug that can turn you into a high roller.
Straight from the Doc has the latest on genes and salt sensitivity.
Dr. Choon advises the cardiac patient to get a good doctor.
Kate Steadman provides tips on how to avoid convalescent boredom. What, no Sudoku?
On the Wards hopes to put off dementia with green tea.
Didn't work then either. Clinical Cases Blog lets us know about Italian balloon endoscopy for weight loss.
My fellow Georgian and paramedic student is frustrated that he cannot enjoy a beer as he does his laundry.

The Recovery Room
But gentle reader, I can go have a beer. The source for the pictures was an article in the Fall 2002 edition of Dartmouth Medical Magazine which has a wealth of information about Dr. Wilder. Sorry for the black and white, I could not find links to color photographs. I hope you have enjoyed Grand Rounds. Next weeks victim---er host----will be Kim at Emergiblog. Want to host? Drop a line to Dr. Genes: Nicholas.Genes(at)umassmed(dot)edu.
As for me....
 |
|
Monday, February 27, 2006
Help the Doctor.....
Grand Rounds Vol II No. 23 will be hosted here tommorrow. Place links in the comment section or email them to me :cut_to_cure(at)hotmail(dot)com. Entries need to be in before 8PM EST tonight.
Here is Dr. Genes' Medscape preview of tomorrows event. |
Grand Rounds Vol II No. 23 will be hosted here tommorrow. Place links in the comment section or email them to me :cut_to_cure(at)hotmail(dot)com. Entries need to be in before 8PM EST tonight.
Here is Dr. Genes' Medscape preview of tomorrows event. |
Sunday, February 26, 2006
Parker's Corollary to the ADS Theorem.....
The Aggravated Surgeon has an excellent post about the "new math" of physician referral. In this particular proof the sum comes out to five million dollars. The Aggravated one opines:
Here is my contribution to the theorem:
Or as the wise man says "figures can't lie but liars can figure". |
The Aggravated Surgeon has an excellent post about the "new math" of physician referral. In this particular proof the sum comes out to five million dollars. The Aggravated one opines:
Having experienced this type of behavior first hand on more than a few occasions, I wonder what the effect of this ruling will have on physicians who have more than a medical relationship with other specialists, or with labs/x-ray facilities/outpatient surgery units etc, for that matter.
Here is my contribution to the theorem:
PCP in multispecialty group practice + insured/daytime/uncomplicated patient = referral to "in group" surgeon.
but
PCP in multispecialty group practice + uninsured/night/weekend/complicated patient = referral to "on call" surgeon.
Or as the wise man says "figures can't lie but liars can figure". |
Grab Your Gun.....
From The Virginian-Pilot:Bill would bar doctors from asking about guns:
More:
The NRA supports the bill:
Like many of us Dr. Ellwood may be the belong to a national group that does not necessarily share her outlook on such things. Now while the AAP has recommendations about water safety, they do not advocate banning swimming pools, bath tubs, or five-gallon buckets. This despite the fact that in 2003 there were about eight times as many accidental deaths from drowning than from firearms in the population aged 1 to 18.
H/T Volokh. |
From The Virginian-Pilot:Bill would bar doctors from asking about guns:
A pediatrician who asks a child's parent about firearms in their home could lose his or her license or be disciplined under legislation being considered by a Senate committee today.
The bill would prohibit health care professionals from asking a patient about gun possession, ownership or storage unless the patient is being treated for an injury related to guns or asks for safety counseling about them.
More:
The legislation is opposed by The Virginia Chapter of the American Academy of Pediatrics because it blocks a common practice by medical professionals to inquire about gun ownership and safety when they go over a safety checklist with parents during a child's regular checkups from birth to puberty.
"We saw the bill but presumed no one in their right mind would put it through," said Dr. Leslie Ellwood, chapter president. "We thought it was such an unusual bill that anyone with common sense wouldn't pass it."
The NRA supports the bill:
The National Rifle Association supports the bill because it will protect gun owners "from intrusive, unnecessary questions from medical professionals," according to the NRA Institute for Legislative Action Web site.Dr. Parker has to call "b.s." on this one. All one would have to say is "it's none of your business". But the NRA is not the only one that is setting off the BS alarm:
"We don't have an opinion or issue an opinion on guns," Ellwood said. "We don't say it is a bad thing to have around children. Our plan is always to find out how the guns are managed in the household so they are safe."Apparently Dr. Ellwood doesn't read the position papers put out by her national organization. From the American Academy of Pediatrics:AMERICAN ACADEMY OF PEDIATRICS: Firearm-Related Injuries Affecting the Pediatric Population .
The AAP makes the following recommendations, which reaffirm and expand on the 1992 policy statement:emphasis mine.
1. The AAP affirms that the most effective measure to prevent firearm-related injuries to children and adolescents is the absence of guns from homes and communities.
a) Firearm regulation, to include bans of handguns and assault weapons, is the most effective way to reduce firearm-related injuries.
b) Pediatricians and other child health care professionals are urged to inform parents about the dangers of guns in and outside the home. The AAP recommends that pediatricians incorporate questions about guns into their patient history taking and urge parents who possess guns to remove them, especially handguns, from the home. Loaded firearms and unlocked firearms and ammunition represent a serious danger to children and adolescents. At especially high risk are adolescents who have a history of aggressive and violent behaviors, suicide attempts, or depression
Like many of us Dr. Ellwood may be the belong to a national group that does not necessarily share her outlook on such things. Now while the AAP has recommendations about water safety, they do not advocate banning swimming pools, bath tubs, or five-gallon buckets. This despite the fact that in 2003 there were about eight times as many accidental deaths from drowning than from firearms in the population aged 1 to 18.
H/T Volokh. |
Tuesday, February 21, 2006
Grand Rounds Vol II No. 22....
Hosted this week by Dr. Andy.
Grand Rounds will be hosted for the third time here next week. Please send submissions along to: cut_to_cure-at-hotmail-dot-com. |
Hosted this week by Dr. Andy.
Grand Rounds will be hosted for the third time here next week. Please send submissions along to: cut_to_cure-at-hotmail-dot-com. |
Tuesday, February 14, 2006
A Valentine's Day gift...
More original than candy and flowers.....
Fits as well as a PajamaGram....(it is, after all, a blog)
Full of double entendre, just like a Vermont Teddy Bear advertisement....
Just perfect: Grand Rounds Vol. II No. 21 hosted by Maria |
More original than candy and flowers.....
Fits as well as a PajamaGram....(it is, after all, a blog)
Full of double entendre, just like a Vermont Teddy Bear advertisement....
Just perfect: Grand Rounds Vol. II No. 21 hosted by Maria |
Really, there is No Spoon......
Your Ultimate Sci-Fi Profile II: which sci-fi crew would you best fit in? (pics)
created with QuizFarm.com |
 |
| You scored as Nebuchadnezzar (The Matrix). You can change the world around you. You have a strong will and a high technical aptitude. Is it possible you are the one? Now if only Agent Smith would quit beating up your friends. |
Your Ultimate Sci-Fi Profile II: which sci-fi crew would you best fit in? (pics)
created with QuizFarm.com |
Monday, February 13, 2006
Tales from the Trauma Service XVI.....
20-ish youn man struck by a car. Diminished level of consciousness upon arrival and is intubated by the ED physician. His initial CXR:
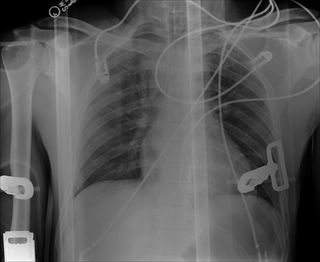
Read as negative by the radiologist. The mediastinum is a little wide, but less than 8 cm. Off to CT he goes:
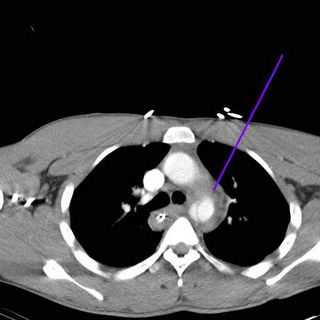
Looky here. The blue line indicates an intimal flap. Off to aortography:

A dissection distal to the left subclavian artery. The list of "classical" radiographic findings suggestive of aortic dissection are:
Additionally anywhere from 3 to 20 percent of patients with normal CXR can have an aortic injury, depending on who you read. This young man was transferred to a referral center (my cardiothoracic coverage was unavailable) and underwent open repair of his injury without complication. |
20-ish youn man struck by a car. Diminished level of consciousness upon arrival and is intubated by the ED physician. His initial CXR:
Read as negative by the radiologist. The mediastinum is a little wide, but less than 8 cm. Off to CT he goes:

Looky here. The blue line indicates an intimal flap. Off to aortography:

A dissection distal to the left subclavian artery. The list of "classical" radiographic findings suggestive of aortic dissection are:
1) Widened mediastinum
2) Loss of aortic knob
3) Tracheal deviation to right
4) Loss of aortic-pulmonary window
5) Depression of left mainstem bronchus
6) Widened paratracheal stripe
7) Apical cap
8) Left hemothorax without rib fracture (also indicative of esophageal injury)
9) Deviation of NG tube
10) Fracture of scapula or first/second rib
Additionally anywhere from 3 to 20 percent of patients with normal CXR can have an aortic injury, depending on who you read. This young man was transferred to a referral center (my cardiothoracic coverage was unavailable) and underwent open repair of his injury without complication. |
Tuesday, February 07, 2006
Monday, February 06, 2006

Sunday, February 05, 2006
Money or Justice II.....
From today's Atlanta Journal-Constitution:Malpractice award caps hamper some victims:
More...
So again, is it money or justice? |
From today's Atlanta Journal-Constitution:Malpractice award caps hamper some victims:
The repetition of pulling large sheets of chewing gum from an assembly line, cracking them in half and heaving them into a machine at the nearby Wrigley factory took its toll on Pat Wright.More....
After more than 20 years in the factory, she could hardly raise her left arm above her shoulder and couldn't bear to lie on it at night.
She finally went under the knife in 2003, but after the surgery she still felt pain. Early last year, another surgeon found the problem: about a half-dozen bright blue metal sutures that had mistakenly been left in her shoulder.
Ever since, Wright has sought an attorney to take her malpractice case, but those she's talked to have refused, citing a new state law that puts a $350,000 cap on jury awards for a malpractice victim's pain and suffering.
Because it can easily cost $100,000 to get a malpractice case to trial, the gamble simply isn't worth it for attorneys in Georgia anymore, and some of the same lawmakers who backed the cap are wondering if the law is too extreme.
Just after Wright learned about the sutures in her shoulder, state lawmakers in Atlanta were overhauling Georgia's medical malpractice laws.Doesn't any damage award put "arbitrary price on a victim's life"? It seems that lawyers are interested only if the price is right.
Following the model of states including Texas and California, Georgia's Republican-led Legislature capped jury awards and made it harder for emergency room patients to win malpractice awards by placing a higher burden of proof on the plaintiffs.
Gov. Sonny Perdue signed the bill into law at an Atlanta hospital, surrounded by applauding doctors and administrators, saying it would improve access to health care throughout the state.
Doctors and hospitals contended the measure, dubbed "civil justice reform," would suppress rising malpractice insurance rates. They said doctors were leaving Georgia --- especially rural areas --- at an alarming pace and told lawmakers it would encourage doctors to stay.
Business lobbies, too, threw their weight behind the bill because it encourages early out-of-court settlements and penalizes parties who file frivolous lawsuits.
But trial lawyers argued that limiting damage awards puts an arbitrary price on a victim's life, and that the state's medical insurer fostered a false crisis by driving up premiums in a market with no competition.
The Medical Association of Georgia, one of the most vocal supporters of tort reform, said the law has transformed the state into a favorable environment for doctors. Anecdotal evidence shows fewer malpractice claims filed, and those that were have been settled more quickly, said David Cook, the group's executive director.So she is upset with both her physicians and her lawyers.
Cook added that steadying malpractice premiums have also stemmed the flow of doctors leaving the state.
Pat Wright said she's one of the unintended consequences of the law.
Since he metal sutures were found in her shoulder, she's gone to at least six attorneys. Each has turned her down, citing the new law.
The two-year statute of limitations on her case may have run out, but since the sutures were only found last year, lawyers have told her she's still got a case. She just can't find one to take it.
"I don't feel like I've been done right," she said. "Somebody should've taken my case."
More...
Others have had problems finding attorneys, too. Willie Davis' wife, Janie, died of a ruptured aorta minutes after leaving a hospital in Perry, a victim of what he says was a misdiagnosed heart condition. Since then, he's been told by six lawyers that they're unwilling to handle his case.Imagine the hue and cry if physicians and hospitals refused service to patients in their direst hour of need, because they couldn't make money off of the transaction. Physicians would be rightly vilified and scorned. But are attorney's held to the same standard? The bad guys aren't the lawyers in this article, but the physicians and legislators trying to solve a problem.
Atlanta attorney Joe Weeks said that two years ago he probably would have represented Davis, but not under the law as it is now.
Janie Davis was 68, a homemaker with no lost wages to recover, no medical bills to repay. "All we had is the value of her life. And the Georgia Legislature said the value of her life is $350,000," Weeks said.
Considering the cost of taking such a case to trial, Weeks said, it wouldn't be worth it.
So again, is it money or justice? |
Saturday, February 04, 2006
ACS to take Ball and Go Home.....
From a reader:Surgeons to boycott Georgia:
What egregious policy? Read on:
Taking the broader view, general surgeons are at a disadvantage in Georgia compared to other surgical specialists. They should be allowed to open their own ambulatory surgery centers. What I see in the future is hospitals hiring their own surgeons, the "surgical hospitalist" to provide coverage for their emergency rooms. |
From a reader:Surgeons to boycott Georgia:
In the latest twist of a long-standing health-care debate, a national group of doctors is boycotting Georgia over the state's laws governing which types of doctors can operate outpatient surgery centers.
The American College of Surgeons, which represents more than 70,000 surgeons, sent letters to Gov. Sonny Perdue and the Georgia Chamber of Commerce saying that it will not consider Georgia as a site for any future conventions or meetings until the state changes its "egregious policy."
What egregious policy? Read on:
The policy causing the controversy stems from Georgia's system for regulating the expansion of health-care services, which is known as the certificate-of-need or CON program.This is a legislative priority of the Medical Association of Georgia. The hospitals don't like the idea of "going around" a CON commission to get this done:
In Georgia, physicians who are considered single-specialty, such as orthopedic or plastic surgeons, can operate ambulatory surgery centers without having to go through the lengthy and often-contentious CON process. But general surgeons are not considered to be single-specialty.
The commission was given two years to do its job, and has been holding monthly meetings since last summer. CON commission members have said that they would not propose any changes until 2007. But health-care insiders are speculating that a bill could be proposed this year specifically on this issue of general surgeons.The ACS hasn't held a meeting in Georgia in years. There was apparently a move to have the 2007 clinical Congress held in Atlanta with the availability of New Orleans in question:
That troubles many hospitals.
"They're trying it to pre-empt the work of the CON commission," said Veazey of the Georgia Alliance of Community Hospitals. "The CON commission was set up to look at all these issues. It's the obligation of the commission to look at all aspects of CON."
Hospitals say it is essential because hospitals often treat patients who cannot pay and often get reimbursed less than their costs.
The group also recently declined to let the Atlanta Convention & Visitors Bureau bid on hosting the group's annual convention, which attracts 15,000 to 18,000 attendees. The convention has a direct economic impact of $10 million to $12 million, according to the American College of Surgeons.According to the ACS site New Orleans is to be dropped in 2010 for Washington D.C.
Taking the broader view, general surgeons are at a disadvantage in Georgia compared to other surgical specialists. They should be allowed to open their own ambulatory surgery centers. What I see in the future is hospitals hiring their own surgeons, the "surgical hospitalist" to provide coverage for their emergency rooms. |

Wednesday, February 01, 2006
Tales of The Trauma Service XV
Young man is a unrestrained back seat passenger in a MVC. CT shows an small intracranial bleed. No other injuries are found. He is awake and alert. A foley is not placed, and since this was one of my partner's cases, I am unsure if he underwent one of those new-age evaluations. He then began to complain of urgency and the inability to void. A foley was unable to be passed and his proximal thigh began to swell. Based on all this a cystogram was ordered:

The black lines represent the CT contrast in his bladder. The blue line represents extravasation of contrast from a urethral injury. He underwent bedside percutaneous cystostomy tube placement and was discharged to home with urologic follow-up on postinjury day six.
The mechanism? Probably the so-called "straddle injury" seen here:
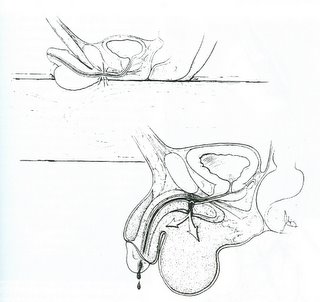
The urethra is trapped between the symphisis pubis and an inflexible object. This injury can result from playground injuries as well.
Young man is a unrestrained back seat passenger in a MVC. CT shows an small intracranial bleed. No other injuries are found. He is awake and alert. A foley is not placed, and since this was one of my partner's cases, I am unsure if he underwent one of those new-age evaluations. He then began to complain of urgency and the inability to void. A foley was unable to be passed and his proximal thigh began to swell. Based on all this a cystogram was ordered:

The black lines represent the CT contrast in his bladder. The blue line represents extravasation of contrast from a urethral injury. He underwent bedside percutaneous cystostomy tube placement and was discharged to home with urologic follow-up on postinjury day six.
The mechanism? Probably the so-called "straddle injury" seen here:
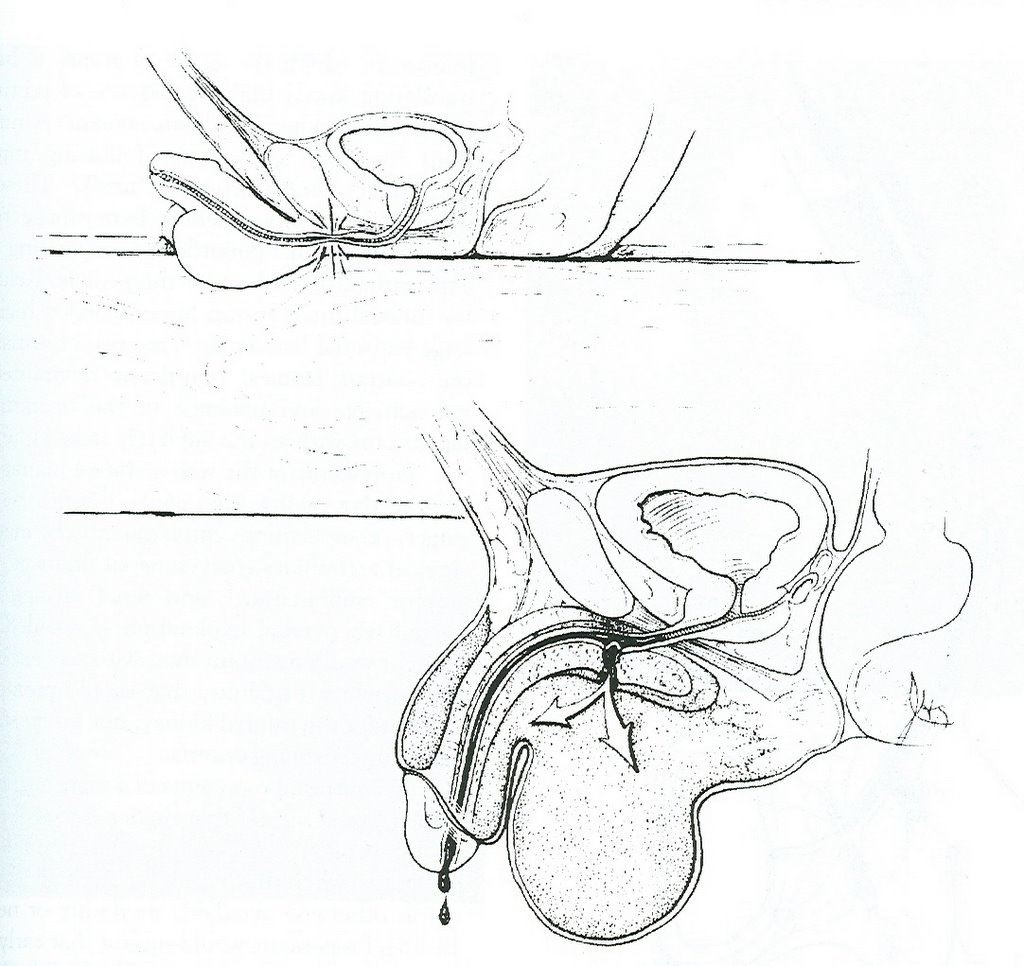
The urethra is trapped between the symphisis pubis and an inflexible object. This injury can result from playground injuries as well.
Labels: Tales from the Trauma Service
|![]()





