Friday, January 27, 2006
Happy Birthday Wishes....
226 candles for theUniversity of Georgia's birthday cake.

Composer of some repute Wolfgang Amadeus Mozart would be 250 years old today.

Also some lawyer guy named John Roberts turns 51.
Why do I care? I was born today just slightly later than the above mentioned. |
226 candles for theUniversity of Georgia's birthday cake.
Composer of some repute Wolfgang Amadeus Mozart would be 250 years old today.
Also some lawyer guy named John Roberts turns 51.

Why do I care? I was born today just slightly later than the above mentioned. |
Wednesday, January 25, 2006
Vroom....Vrooom.....
I'm a Porsche 911!

You have a classic style, but you're up-to-date with the latest technology. You're ambitious, competitive, and you love to win. Performance, precision, and prestige - you're one of the elite,and you know it.
Take the Which Sports Car Are You? quiz.
|
Goodbye to the Finger Wave...
The latest burning controversy in trauma surgery: perform the SMA-1 or not? From the Journal of Trauma: Reasons to Omit Digital Rectal Exam in Trauma Patients: No Fingers, No Rectum, No Useful Additional Information. From the abstract:
Snippets from the discussion:
Good study and good points are made. Certainly goes against the old "no finger or no rectum" being the only exceptions to performing a rectal exam. It will be interesting to see how much this takes off. But for now, join in the chorus of Moon River. |
The latest burning controversy in trauma surgery: perform the SMA-1 or not? From the Journal of Trauma: Reasons to Omit Digital Rectal Exam in Trauma Patients: No Fingers, No Rectum, No Useful Additional Information. From the abstract:
Background: Performance of digital rectal examination (DRE) on all trauma patients during the secondary survey has been advocated by the Advanced Trauma Life Support course. However, there is no clear evidence of its efficacy as a diagnostic test for traumatic injury. The purpose of this study is to analyze the value of a policy mandating DRE on all trauma patients as part of the initial evaluation process and to discern whether it can routinely be omitted.For a year trauma patients underwent DRE's and a data collection tool was used and the diagnostic acumen of both were compared. Here is the data sheet:
Methods: Prospective study of patients treated at a Level I trauma center. Clinical indicators other than DRE (OCI) denoting gastrointestinal bleeding (GIB), urethral disruption (UD), or spinal cord injury (SCI) were sought and correlated with DRE findings suggesting the same. Impression of the examining physician as to the need and value of DRE was also studied. Patients with a Glasgow Coma Scale Score (GCS) of 3 and pharmacologically paralyzed were excluded from the SCI analyses. UD analysis included only males.
Results: In all, 512 cases were studied (72% male, 28% female) ranging in age from 2 months to 102 years. Thirty index injuries were identified in 29 patients (6%), 17 SCI (3%), 11 GIB (2%), and 2 UD (0.4%). DRE findings agreed positively or negatively with one or more OCI of index injuries in 93% of all cases (92% seeking SCI, 90% seeking GIB, 96% seeking UD). Overall, negative predictive value of DRE was the same as that of OCI, 99% (SCI 98% versus 99%, GIB, 97% versus 99%, UD both 100%). Positive predictive value for DRE was 27% and for OCI 24% (SCI 47% versus 44%, GIB 15% versus 18%, UD 33% versus 6%). Efficiency of DRE was 94% and OCI was 93%. For confirmed index injuries, indicative DRE findings were associated with 41% and OCI 73% (SCI 36% versus 79%, GIB 36% versus 73%, UD 50% versus 100%). OCIs were present in 81% of index injury cases. In all index injury cases where OCIs were absent, positive DRE findings were also absent. DRE was felt to give additional information in 5% of all cases and change management in 4%. In cases where the clinician felt DRE was definitely indicated (29%) it reportedly gave no additional information in 85% and changed management in 11%.
Conclusion: DRE is equivalent to OCI for confirming or excluding the presence of index injuries. When index injuries are demonstrated, OCI is more likely to be associated with their presence. DRE rarely provides additional accurate or useful information that changes management. Omission of DRE in virtually all trauma patients appears permissible, safe, and advantageous. Elimination of routine DRE from the secondary survey will presumably conserve time and resources, minimize unpleasant encounters, and protect patients and staff from the potential for further harm without any significant negative impact on care and outcome.
Snippets from the discussion:
This study demonstrates that DRE is equivalent to OCI for confirming or excluding the presence of index injuries, and is of limited value in the initial assessment of trauma patients. DRE rarely provided additional accurate or useful information that changed patient management. Clinical acumen based on other information, short of DRE results, appears to be a safe and accurate method of ruling in, or ruling out, an index injury thereby avoiding this unpleasant encounter.The fact that it rolls downhill can affect the diagnostic utility of the DRE:
In this study, when all cases are considered, the NPV, PPV, and efficiency (which is essentially a measure of accuracy) of DRE and OCI are no different, potentially making one or the other expendable. Furthermore, in cases with confirmed index injury, the more accurate tool proved to be OCI. In all index injury cases where OCI were falsely negative, DRE was falsely negative as well. Therefore, no index injury would have been missed by omitting DRE that would also not be missed by relying on OCI alone. However, omission of DRE would have avoided acquisition of false-negative or false-positive information in 31 patients or 6% of the entire sample versus 21 or 4% for OCI. Of greater note, and perhaps clinical importance, is the significantly higher false-negative examination rate (63%) for DRE compared with OCI (22%) in patients with confirmed index injury.
One factor that may contribute to the propensity of DRE to yield less than useful or accurate information is that it is generally relegated to the least experienced member of the trauma team (at least in academic centers), which is often a medical student. This may stem from the perceived menial nature of the task or a genuine effort to provide a complete educational experience. The issue of poor interrater reliability in determining normal and abnormal DRE has been raised. Further, other investigators have found difficulty even among experienced examiners in determining normal and abnormal rectal tone as confirmed by manometry.There is also the concern of violence or litigation associated with rectal exams:
The occurrence of violence in the emergency department setting, despite being under reported, is well described. In one study, 36% of surgical staff and 30% of emergency department staff were assaulted. Verbal assaults are more common than physical assaults. The profile of both perpetrator and victim of violence fit well with the trauma patient and the physician relegated to the task of DRE, at least in academic centers. The perpetrator is usually young, male, intoxicated, or a substance abuser. Doctors are less likely to be victims than nurses, but those physicians who are victims tend to be younger and less experienced. Circumstances precipitating assault are not well described. Although DRE is never specifically implicated, one study does describe a significant correlation with averse stimulation of the patient. It would be reasonable to assume that DRE falls into that category. Although there were no documented episodes of physical assault on the examiner related to DRE in this current study, anecdotally, instances of animated protest and verbal abuse were not uncommon. This is consistent with the cited literature.
DRE, if misunderstood or poorly performed can lead to litigation, or other administrative actions initiated as a result of complaints. A noteworthy level of emotional and physical discomfort associated with DRE has also been described,which may precipitate a less than optimal doctor, patient encounter, and heightened potential for the above mentioned occurrences. There are also small but not insignificant or inconsequential risks of adverse patient events associated with DRE related to rectal injury or other conditions. Again, although such actual or potential occurrences are rare, avoidance of even the smallest of risks seems sensible from a number of standpoints if an equivalent screening process that is less provocative can be substituted for DRE.
Good study and good points are made. Certainly goes against the old "no finger or no rectum" being the only exceptions to performing a rectal exam. It will be interesting to see how much this takes off. But for now, join in the chorus of Moon River. |
Sunday, January 22, 2006
I Have Trouble Remembering Which End to Use......
The stethoscope enters the 21st century: When a Heart Beats In a Noisy Hospital,Who Can Hear It?
The stethoscope has come a long way in its' near 200 years...
The stethoscope enters the 21st century: When a Heart Beats In a Noisy Hospital,Who Can Hear It?
At a medical conference in Florida last March, about 100 cardiologists found themselves stooped over little Plexiglas cubes, listening intently with a newfangled stethoscope.
Coming from the "sound boxes" were recorded heart and lung sounds, plus a lot of annoying hospital clatter. The doctors were conducting the equivalent of a taste test, comparing an experimental electronic stethoscope made by 3M Co. to traditional, acoustic stethoscopes made by the same company. The experimental stethoscope is designed to muffle outside noise.
It's a loud world. And the racket is rising in hospitals, according to recent research done by Johns Hopkins University in Baltimore. Acoustical engineers there took sound readings in the immediate vicinity of hospital patients and then compared results with those of historical noise studies. Since 1960, researchers found, average daytime hospital sound levels have risen from 57 decibels (roughly equivalent to a churning washing machine) to 72 (more like a grinding garbage disposal) today.
It's remarkably difficult to design a stethoscope that filters out environmental noise while still amplifying the subtle, vital sounds of the inner anatomy. For 3M and its smaller scope-making rivals, the prize is a chunk of a fairly big market. Global stethoscope sales are between $125 million and $150 million, with about half of the sales in the U.S. Relatively new, electronic scopes represent less than 10% of the market, 3M estimates.
The stethoscope has come a long way in its' near 200 years...
One of medicine's trustiest diagnostic devices, the stethoscope was invented in 1816 by a French physician, Rene Theophile Hyacinthe Laennec. His first model was simply a perforated wooden cylinder. Another clever inventor in 1880 made a trumpet-shaped model with a rubber end that doubled as a reflex hammer to rap on knees. Around the same time, the binaural, or twin-ear, stethoscope came onto the market, a major advance in reducing background noise.Pricey tools they are:
But noise -- including human voices, the whoosh of air conditioning and heating systems, and the sounds of medical monitors -- continues to confound. The problem got worse in recent years after stethoscope companies tried to amplify the inner rhythms doctors really want to hear but inadvertently also raised the level of ambient racket.
Stethoscopes have long captured the body's wind and percussion sections: the lungs and heart. The instruments are either acoustic or electronic. The electronic ones amplify the sound. There were numerous attempts to design and patent amplifying stethoscopes in the early 1900s. But they didn't catch on until the late 1990s when they could be powered by small batteries.
A handful of companies have introduced electronic models in recent years, including the Echo Amplified sold by Trimline Medical Products Corp. and the Master Elite from Welch Allyn Inc. Electronic scopes tend to be used by cardiologists and respiratory specialists. Their manufacturers usually make some claim about filtering out environmental noise. The newer scopes certainly help amplify very faint sounds: gentle heart murmurs and subtle crackles and wheezes that can indicate heart disease, pneumonia and other serious ailments.
A doctor in Norway using one of the electronic scopes happened upon a high-frequency wheeze in a patient who was later found to have bronchial cancer. In a 2001 research paper, the doctor, Hasse Melbye, wrote: "I could scarcely have heard this sound with a [standard] stethoscope."
His stethoscope was made by Welch Allyn, a medical-instruments company in Skaneateles Falls, N.Y., which introduced the Master Elite Plus in 2000. The device's $446 price was easily twice that of many high-end stethoscopes. Garden-variety stethoscopes can run $65 or less. Then in 2003, Welch Allyn unveiled a moderately priced Master Elite for $245. The company generated some buzz by advertising that the scope used patented electronic-sensor technology to filter out unwanted noise.3M has come out with a model as well:
Rival 3M, which markets the industry-leading Littmann electronic stethoscope, had its work cut out. Its researchers already had attacked noise-damping from several angles, at one point with special ear tips (patent no. 5,824,968) that made a tighter seal in the doctor's ear canal. 3M researchers next sounded out Bang & Olufsen, the maker of fancy sound systems. Working with the Danish company's acoustical specialists, the 3M scientists got busy designing a stethoscope that could gather environmental noise separately from the noises created by the patient.Still a little pricey for my tastes. But if the price falls, I certainly can see the use for such a device in the trauma room. Tough to evaluate for Beck's Triad in the noisy ED. |
To draw in sound from the air, designers experimented with a thin slit (0.040 of an inch) carved around the diameter of the chestpiece. Ambient noise, say a squeaky gurney, enters the device from the outside through that hole. There, it meets the same noise, which has been conducted through the patient's body. Because the scope is receiving the same vibrations from two different places, it cancels them out, leaving heart and lung sounds audible.
To satisfy the Food and Drug Administration, 3M began testing the new stethoscope on people about a year ago. The company, which makes products from Post-it notes to Scotch tape, brought doctors and patients to its headquarters in St. Paul, Minn. In a reverberation room -- a concrete chamber about the size of a one-car garage -- scientists re-created hospital cacophony from recorded sounds. Bells rang. Carts rolled. Bed rails squeaked. Respirators hummed. Voices mumbled incoherently in what 3M calls "hospital babble."
Heart specialists and other doctors conducted exams on real patients suffering from a variety of conditions, including a heart murmur and asthma. As doctors pressed stethoscopes to the patients, researchers assaulted the room with volumes of background noise from 60 to 80 decibels.
Feeling the new stethoscope sufficiently muffled unwanted noise, 3M next had to persuade doctors. Hospitals typically don't buy stethoscopes in bulk; doctors usually pick their own and pay for them.
3M devised the little sound boxes that cardiologists were bending over at the medical conference in Florida last spring. The plastic cubes were miniature versions of the reverberation room in Minnesota.
3M says tests show that its new stethoscope, introduced in November with FDA approval at a suggested retail price of $374, can reduce ambient noise by 75%.
Tuesday, January 10, 2006
Friday, January 06, 2006
Tales From the Trauma Service XIV.....
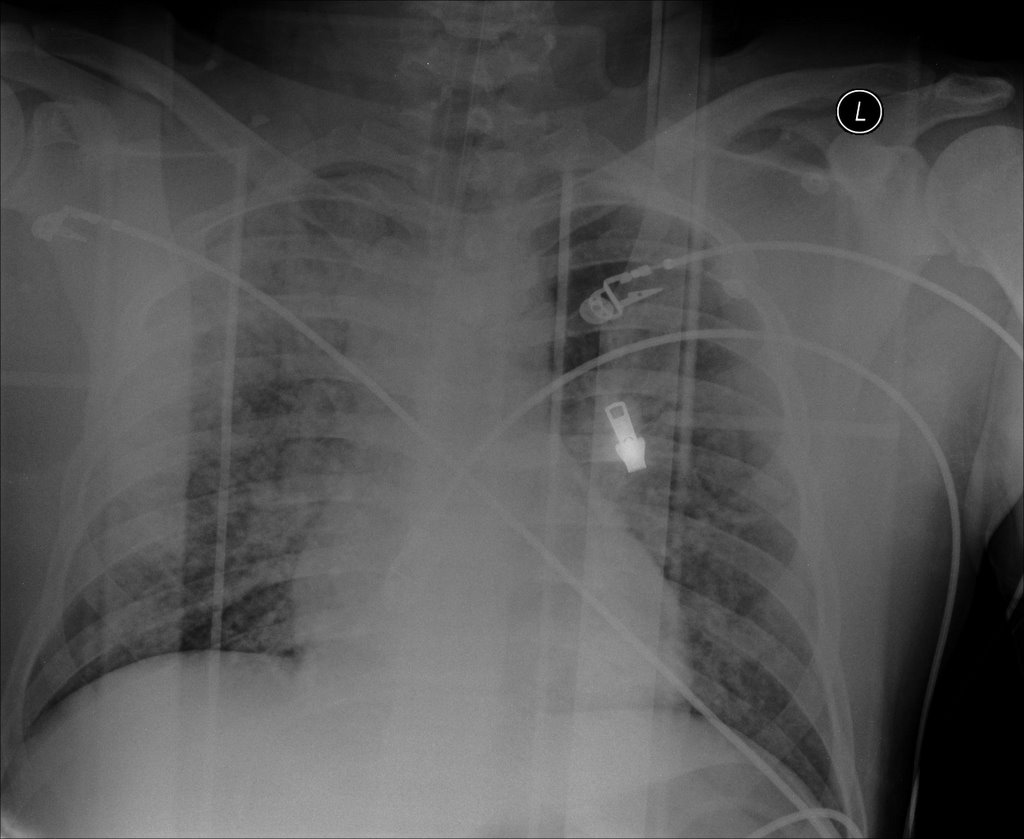
Twenty-ish year old unrestrained driver in MVC. Airlifted from the scene. Intubated with difficulty in the ED. Difficult to oxygenate with a O2 saturation in the 40 to 50 percent range. Here is the CXR:
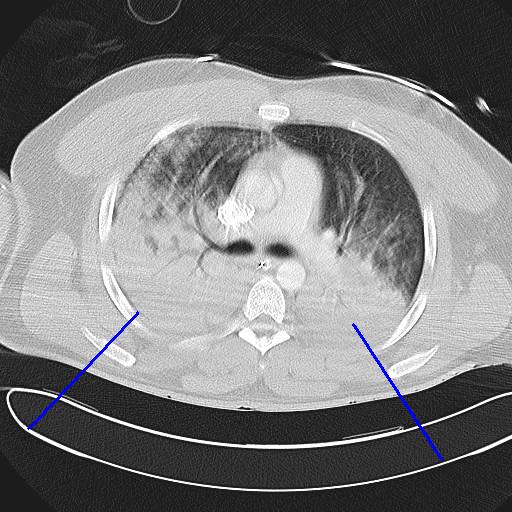
After some vent maneuvers such as increasing PEEP and using pressure control ventilation we are able to raise his saturation to the 70 percent range so we can go to CT:


As you can see there were severe contusions bilaterally. No fluid in the posterior and there is no evidence of a pneumothorax. To add to this young man's woes:


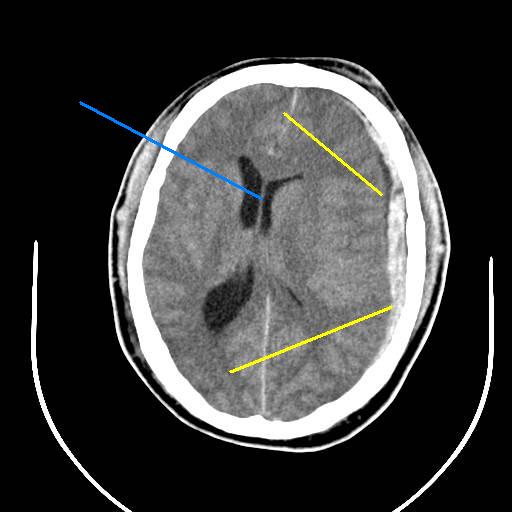
He has a severe subdural and subarachnoid hemorrhage (yellow) and a midline shift (blue. The enemies of head injuries are hypotension and hypoxia. After discussion with the neurosurgeon and anesthesiologist the decsion is made to take him to the OR for a craniotomy and chest tube placement. Chest tubes were placed because of the potential for barotrauma with high pressure ventilation. Try as we might, it took about 16 hours to correct his hypoxia. When oxygen is restored to a previously hypoxic organ (or blood flow is re-established) you can get what is known as a repefusion injury. As oxygen is restored there evolved into what could be described as a body wide re-prefusion injury with hypotension that required high levels of pressor support. His neurologic status continued to decline and his family decided to de-escalate his care and he expired on the fourth hospital day.
Again, somedays you get the bear, somedays the bear gets you.
Twenty-ish year old unrestrained driver in MVC. Airlifted from the scene. Intubated with difficulty in the ED. Difficult to oxygenate with a O2 saturation in the 40 to 50 percent range. Here is the CXR:
After some vent maneuvers such as increasing PEEP and using pressure control ventilation we are able to raise his saturation to the 70 percent range so we can go to CT:
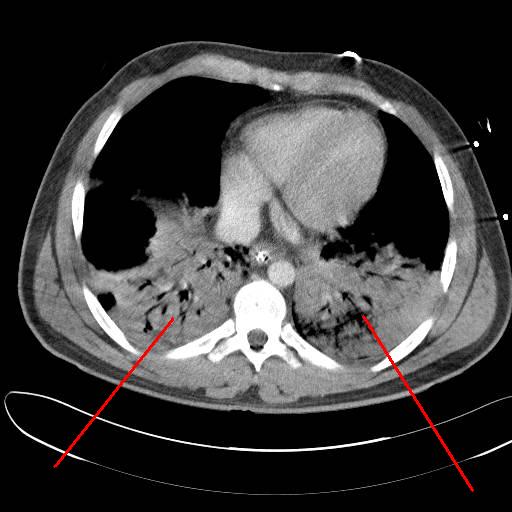
As you can see there were severe contusions bilaterally. No fluid in the posterior and there is no evidence of a pneumothorax. To add to this young man's woes:

He has a severe subdural and subarachnoid hemorrhage (yellow) and a midline shift (blue. The enemies of head injuries are hypotension and hypoxia. After discussion with the neurosurgeon and anesthesiologist the decsion is made to take him to the OR for a craniotomy and chest tube placement. Chest tubes were placed because of the potential for barotrauma with high pressure ventilation. Try as we might, it took about 16 hours to correct his hypoxia. When oxygen is restored to a previously hypoxic organ (or blood flow is re-established) you can get what is known as a repefusion injury. As oxygen is restored there evolved into what could be described as a body wide re-prefusion injury with hypotension that required high levels of pressor support. His neurologic status continued to decline and his family decided to de-escalate his care and he expired on the fourth hospital day.
Again, somedays you get the bear, somedays the bear gets you.
Labels: Tales from the Trauma Service
|Thursday, January 05, 2006
Wednesday, January 04, 2006
Tuesday, January 03, 2006

Georgia 35 West Virginia 38
The first quarter almost made me physically ill. Twenty-eight points in less than fifteen minutes. Georgia closed it to 10 by halftime, but with three turnovers (two leading to Mountaineer touchdowns), Georgia couldn't "finish the drill". And just when you thought that Shockley would have another opportunity to win the game, WVU runs a well-executed fake punt for a first down.
Oh well, just eight months until the Western Kentucky Hilltoppers come to Athens. |
![]()



