Friday, April 29, 2005
An Inspiration to Surgical Residency Program Directors Everywhere....
The Darth Vader Blog
Via Dr. Baggaley |
The Darth Vader Blog
Via Dr. Baggaley |
Tales from the Trauma Service X.....
What a week.
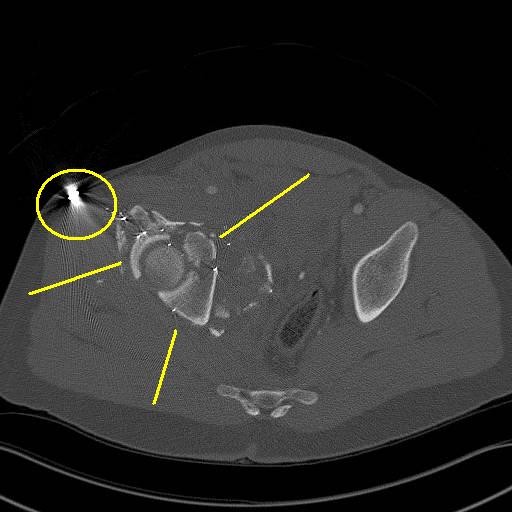
20-ish year old GSW to the back with an entry a L5. Claims he was shot with an AK-47. OK, whatever you say. Mildly hypotensive in the 80's. Responds to some IVF. Initial pelvis film:

That's got to sting. Paperclip marks the entry. He gets two units of packed cells. Off to CT:
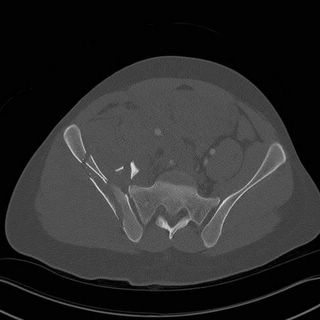
Iliac wing shattered....
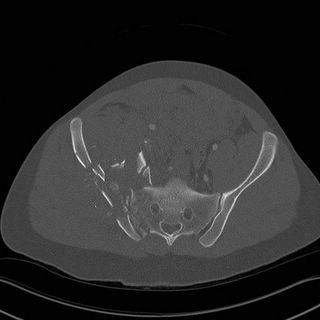
You can see the hematoma displacing the right iliac artery....
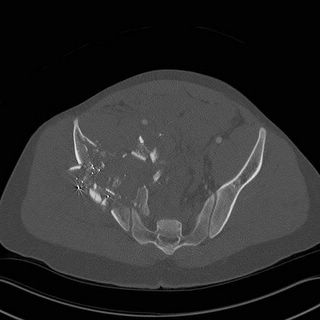
Hell, maybe it was a Kalashnikov that did the deed...

The lines indicate what is left of his acetabulum. There are fragments in the joint space.
The hematoma is easier to see in this window.

See how far the foley balloon and rectum are being pushed to the left.
Fixing this kind of fracture is a large undertaking. He required transfer to a referral facility.
What a week.
20-ish year old GSW to the back with an entry a L5. Claims he was shot with an AK-47. OK, whatever you say. Mildly hypotensive in the 80's. Responds to some IVF. Initial pelvis film:

That's got to sting. Paperclip marks the entry. He gets two units of packed cells. Off to CT:

Iliac wing shattered....

You can see the hematoma displacing the right iliac artery....

Hell, maybe it was a Kalashnikov that did the deed...
The lines indicate what is left of his acetabulum. There are fragments in the joint space.

The hematoma is easier to see in this window.

See how far the foley balloon and rectum are being pushed to the left.
Fixing this kind of fracture is a large undertaking. He required transfer to a referral facility.
Labels: Tales from the Trauma Service
|Thursday, April 28, 2005
Scenes From A Call Weekend.....
Friday a 50-ish struck by a drunken driver. Prolonged extrication with the loss of pulse enroute. The weather was bad so it was about a 15-minute ride in. He arrived still with no pulse. Asystole on the monitor. 8 french femoral sheath inserted and fluids through the rapid infusor. Compressions, epi, and atropine oh my! The ED physician and I agree that we will give one more round of drugs and then call it. He has been down for about 20 minutes at this time.
He then regains a pulse and BP.
Oh $h!t, what do I do?
He maintains a pressure of 110 or so for awhile, FAST shows a small amount of fluid within the abdomen, but not much. I contemplate a trip to CT while he is still stable but he then becomes what the ATLS book calls a "transient responder". As long as the fluids and blood are running in full tilt he is able to maintain a pressure of about 90. His rectal temp is 94. He doesn't appear to be about to arrest again. I consider the options and figure the guy came back from a blunt arrest so the least I ought to do is head to the OR to see if there is anything fixable.
Off we go. Sorry, no pictures.
Found a relatively minor splenic injury and a renal contusion. Had to place an aortic occluder at the start of the case but despite transfusions of blood, FFP and a great deal of crystalliod I could never remove the occluder and have the patient maintain a BP. Since long-term clamping of the aorta at the diaphragmatic hiatus is poorly tolerated I had to call it a day. He died about five minutes after the occluder was removed.
The drunk that went across an interstate-grade median and hit him, and several others got his workup and was hauled to jail.
Saturday was pretty quiet, watching the NFL draft.
Sunday was highlighted by an amputation, this case, and a five month old, unrestrained and in the front seat, involved in a rear-end collision. The latest nominee for mother if the year was arrested for an outstanding warrant as well as for possession of methamphetamine.
The child, fortunately was unhurt. |
Friday a 50-ish struck by a drunken driver. Prolonged extrication with the loss of pulse enroute. The weather was bad so it was about a 15-minute ride in. He arrived still with no pulse. Asystole on the monitor. 8 french femoral sheath inserted and fluids through the rapid infusor. Compressions, epi, and atropine oh my! The ED physician and I agree that we will give one more round of drugs and then call it. He has been down for about 20 minutes at this time.
He then regains a pulse and BP.
Oh $h!t, what do I do?
He maintains a pressure of 110 or so for awhile, FAST shows a small amount of fluid within the abdomen, but not much. I contemplate a trip to CT while he is still stable but he then becomes what the ATLS book calls a "transient responder". As long as the fluids and blood are running in full tilt he is able to maintain a pressure of about 90. His rectal temp is 94. He doesn't appear to be about to arrest again. I consider the options and figure the guy came back from a blunt arrest so the least I ought to do is head to the OR to see if there is anything fixable.
Off we go. Sorry, no pictures.
Found a relatively minor splenic injury and a renal contusion. Had to place an aortic occluder at the start of the case but despite transfusions of blood, FFP and a great deal of crystalliod I could never remove the occluder and have the patient maintain a BP. Since long-term clamping of the aorta at the diaphragmatic hiatus is poorly tolerated I had to call it a day. He died about five minutes after the occluder was removed.
The drunk that went across an interstate-grade median and hit him, and several others got his workup and was hauled to jail.
Saturday was pretty quiet, watching the NFL draft.
Sunday was highlighted by an amputation, this case, and a five month old, unrestrained and in the front seat, involved in a rear-end collision. The latest nominee for mother if the year was arrested for an outstanding warrant as well as for possession of methamphetamine.
The child, fortunately was unhurt. |
Wednesday, April 27, 2005
Academic Medicine in the Wild....
Orac provides points on how to spot various species milling about scientific meetings in his "Field Guide to Biomedical Meeting Creatures" Part One and Part Two.
Don't forget to bring your field glasses! |
Orac provides points on how to spot various species milling about scientific meetings in his "Field Guide to Biomedical Meeting Creatures" Part One and Part Two.
Don't forget to bring your field glasses! |
Sex and the Resident....
The Madman provides another review of Grey's Anatomy which prompts Galen to ask if all surgical residencies are soap operas in the making.
Sorry to say that the residents and attendings weren't shacking up where I trained. Sure some residents "hooked up" with other residents and there was the cliche' of the resident sleeping with the nurse or respiratory therapist. But nothing occurred on the scale of The House of God, by any stretch.
The closest that the department came to that was the wife of a new faculty member my fourth year, who was an OB/GYN attending, was having a rather torrid affair with a student. This particular student was also applying to OB/GYN residencies and the affair was discovered after the faculty member had written letters of recommendation for her lover. The chair then sent letters to all of the programs that the student applied to "explaining" the "situation".
The inevitable threat of a wrongful termination suit resulted in the faculty member coming into work every day, and sitting in her office relieved of her clinical duties until she, and her surgeon husband, found new jobs.
Just like "General Hospital" ain't it? |
The Madman provides another review of Grey's Anatomy which prompts Galen to ask if all surgical residencies are soap operas in the making.
Sorry to say that the residents and attendings weren't shacking up where I trained. Sure some residents "hooked up" with other residents and there was the cliche' of the resident sleeping with the nurse or respiratory therapist. But nothing occurred on the scale of The House of God, by any stretch.
The closest that the department came to that was the wife of a new faculty member my fourth year, who was an OB/GYN attending, was having a rather torrid affair with a student. This particular student was also applying to OB/GYN residencies and the affair was discovered after the faculty member had written letters of recommendation for her lover. The chair then sent letters to all of the programs that the student applied to "explaining" the "situation".
The inevitable threat of a wrongful termination suit resulted in the faculty member coming into work every day, and sitting in her office relieved of her clinical duties until she, and her surgeon husband, found new jobs.
Just like "General Hospital" ain't it? |
Tales from the Trauma Service IX......
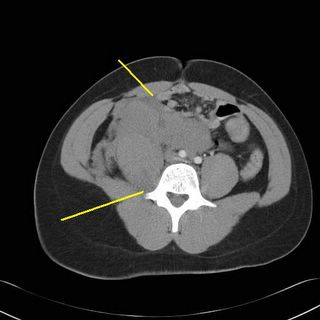
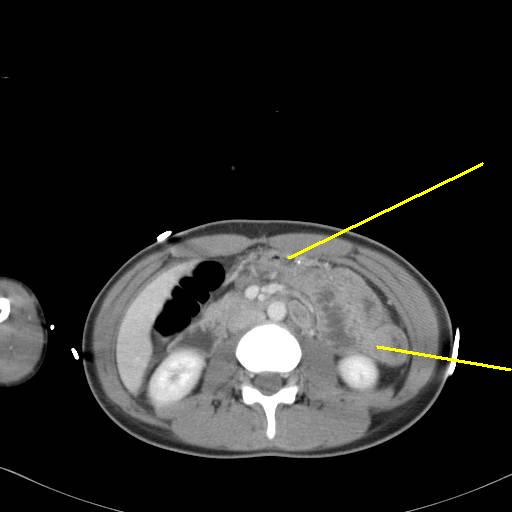
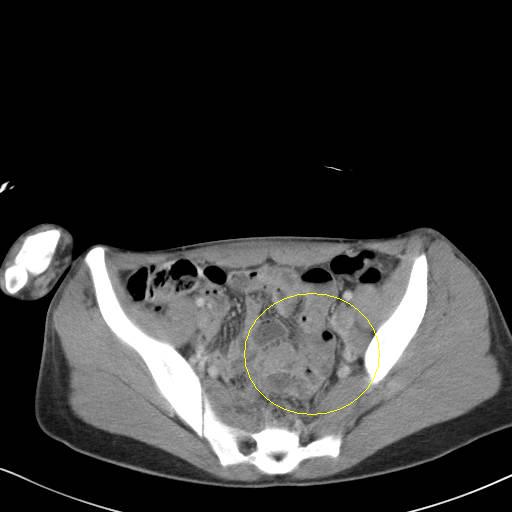
20-ish female in a multi-vehicle MVC. Arrives to the ED in the midst of a grand-mal seizure. Intubated and given sedatives and anti-seizure medications. Gets a CT of head, c-spine, and abdomen pelvis with the following images of note:



This was read out as "unusual attenuation of small bowel which could represent bleeding or inflammation" and "free fluid within pelvis". I can buy the free fluid. The solid organs were "without traumatic injury".
While getting better the main weakness of abdominal CT is the ability to detect small bowel injuries. If this patient had not been intubated and head injured I probably would have done the old "serial exam" routine. Her WBC's were 14.5k and her amylase was at the high end of normal.
Off to the OR.....
Found about 200cc of old-looking blood. Bowel run from the LOT to the rectum without any signs of injury. Liver OK, stomach and pancreas OK, looked at the spleen and:

Left it alone since it was no longer bleeding. I felt guilty about exploring her but I would have felt more guilty about missing the injury.
20-ish female in a multi-vehicle MVC. Arrives to the ED in the midst of a grand-mal seizure. Intubated and given sedatives and anti-seizure medications. Gets a CT of head, c-spine, and abdomen pelvis with the following images of note:

This was read out as "unusual attenuation of small bowel which could represent bleeding or inflammation" and "free fluid within pelvis". I can buy the free fluid. The solid organs were "without traumatic injury".
While getting better the main weakness of abdominal CT is the ability to detect small bowel injuries. If this patient had not been intubated and head injured I probably would have done the old "serial exam" routine. Her WBC's were 14.5k and her amylase was at the high end of normal.
Off to the OR.....
Found about 200cc of old-looking blood. Bowel run from the LOT to the rectum without any signs of injury. Liver OK, stomach and pancreas OK, looked at the spleen and:

Left it alone since it was no longer bleeding. I felt guilty about exploring her but I would have felt more guilty about missing the injury.
Labels: Tales from the Trauma Service
|Thursday, April 21, 2005
Called and Raised.....
Unless some physician behavior is changed I fear that the gains made in tort reform will be lost. I'm not talking about "sloppy medicine" or "bad doctors". I am referring to physicians inability to live up to the perhaps unspoken agreement that assisted passage of tort reform, at least in Georgia.
Look at section I of SB 3, which was signed into law in February (emphasis mine):
Implicit in the above is that, if the problems are fixed, then physicians will return to the ED call schedule. However Big Hospital's plastic surgeons are coming off staff and the urologists and ENT physicians are threatening to do so as well. They recognize the benefits of tort reform but are leaving based on such things as reimbursement and "having to come in in the middle of the night". While those are valid complaints, and similar to one's I have made myself, I fear that we may be penny wise and pound foolish. I fear that if the access problem does not improve that the legislature will undo most of the reforms or use other methods to improve access.
The benefits of tort reform are not only seen in the emergency department but everywhere we treat patients. The opponents of tort reform are well organized and will no doubt pounce on this issue if physicians allow it to do so.
The efforts toward tort reform in other states may suffer as well. Those opposed could point to Georgia and the access problems that remain after tort reform and claim that the main argument for altering the civil justice system is a false one.
Maybe physicians are waiting to see how the inevitable court challenge plays out. Perhaps they are afraid of getting back into it, only to find themselves exposed at a later date if the court overturns some reforms. But I worry that the patience of the public and the legislature may not last that long. |
Unless some physician behavior is changed I fear that the gains made in tort reform will be lost. I'm not talking about "sloppy medicine" or "bad doctors". I am referring to physicians inability to live up to the perhaps unspoken agreement that assisted passage of tort reform, at least in Georgia.
Look at section I of SB 3, which was signed into law in February (emphasis mine):
The General Assembly finds that there presently exists a crisis affecting the provision and quality of health care services in this state. Hospitals and other health care providers in this state are having increasing difficulty in locating liability insurance and, when such hospitals and providers are able to locate such insurance, the insurance is extremely costly. The result of this crisis is the potential for a diminution of the availability of access to health care services and a resulting adverse impact on the health and well-being of the citizens of this state. The General Assembly further finds that certain civil justice and health care regulatory reforms as provided in this Act will promote predictability and improvement in the provision of quality health care services and the resolution of health care liability claims and will thereby assist in promoting the provision of health care liability insurance by insurance providers. The General Assembly further finds that certain needed reforms affect not only health care liability claims but also other civil actions and accordingly provides such general reforms in this Act.The "problem of access" was the rather large club used to bludgeon legislators into giving the physicians of Georgia essentially everything they wanted. Access to services can be lost by physicians closing up shop, or more commonly, refusing to take ED call. The latter was addressed specifically by section X4(b), the section raising the negligence burden for emergency cases: (emphasis mine)
The General Assembly makes the following findings: Georgia hospitals operating dedicated emergency departments are required by both state and federal law to provide examination and treatment to individuals who come to a dedicated emergency department, without regard to the financial or insurance status of such individuals. Hospitals and other health care providers have complied with these laws to their financial detriment and under the well-founded apprehension of increased liability. Due in large part to fear of such liability, hospitals are experiencing extreme difficulty attracting a sufficient number of physicians and other health care professionals to maintain an effective team of professionals, including on-call physicians, to provide needed care and assistance to citizens of this state. As a result, many hospitals are being forced to close their emergency departments or forgo other needed improvements in order to financially support such emergency services and their attendant liability. The shortage of these emergency providers poses a serious threat to the health, welfare, and safety of the citizens of Georgia.
Implicit in the above is that, if the problems are fixed, then physicians will return to the ED call schedule. However Big Hospital's plastic surgeons are coming off staff and the urologists and ENT physicians are threatening to do so as well. They recognize the benefits of tort reform but are leaving based on such things as reimbursement and "having to come in in the middle of the night". While those are valid complaints, and similar to one's I have made myself, I fear that we may be penny wise and pound foolish. I fear that if the access problem does not improve that the legislature will undo most of the reforms or use other methods to improve access.
The benefits of tort reform are not only seen in the emergency department but everywhere we treat patients. The opponents of tort reform are well organized and will no doubt pounce on this issue if physicians allow it to do so.
The efforts toward tort reform in other states may suffer as well. Those opposed could point to Georgia and the access problems that remain after tort reform and claim that the main argument for altering the civil justice system is a false one.
Maybe physicians are waiting to see how the inevitable court challenge plays out. Perhaps they are afraid of getting back into it, only to find themselves exposed at a later date if the court overturns some reforms. But I worry that the patience of the public and the legislature may not last that long. |
Wednesday, April 20, 2005

Tuesday, April 19, 2005
Monday, April 18, 2005
Dr. Parker's Game Reviews......
First off, Star Wars Republic Commando, a squad-based first person shooter based in the Star Wars universe during the time between Attack of the Clones and Revenge of the Sith. The squad controls are easy to use and the team AI is very good. The only drawback I could see was the game was a very short one. Highly recommended.
Lastly, the acclaimed WW2 tactical shooter: Brothers in Arms:Road to Hill 30. This game was highly touted for its' realism both in tactics and terrain. This game was to take the squad action of Call of Duty a step further by placing control of the squad under your command. Friendly AI was very good. Some problems I had with the game was the inability to kill enemies even at very close range. There was little to no variation in the actions of the enemy. The language is coarse. If you enjoy WW2 themed games, you will enjoy it, if not you may be disappointed.
Ahh, now back to Half-Life 2. |
First off, Star Wars Republic Commando, a squad-based first person shooter based in the Star Wars universe during the time between Attack of the Clones and Revenge of the Sith. The squad controls are easy to use and the team AI is very good. The only drawback I could see was the game was a very short one. Highly recommended.
Lastly, the acclaimed WW2 tactical shooter: Brothers in Arms:Road to Hill 30. This game was highly touted for its' realism both in tactics and terrain. This game was to take the squad action of Call of Duty a step further by placing control of the squad under your command. Friendly AI was very good. Some problems I had with the game was the inability to kill enemies even at very close range. There was little to no variation in the actions of the enemy. The language is coarse. If you enjoy WW2 themed games, you will enjoy it, if not you may be disappointed.
Ahh, now back to Half-Life 2. |
Sunday, April 17, 2005
Consent....
In a recent post Kevin asks, in reference to a recurrent laryngeal nerve injury: Isn't part of informed consent acceptance of that risk? In some ways it is but it is not a shield from liability by any means. As one of his commenters put it:
Informed consent does provide some protection for common, "low impact" complications like wound infections. The infection rare from an uncomplicated appendectomy is about ten percent, but the treatment for it is simple. Since patients are made aware of this my liability exposure is low. Informed consent also allows for the unexpected. From the "boilerplate" consent form used in my office:
This allows for the treatment of the unexpected. Such as the colon malignancy found during exploratory laparotomy for trauma. Sometimes a colostomy has to be constructed when not expected. Under the statement above, as well as listing some circumstances as "special risks", you can be covered.
There is also the school of thought that informed consent cannot be completely given freely. They maintain that patients give consent under duress because if they do not give it, they will be denied surgery, so they will sign anything to relive their pain.
A discussion about informed consent may be found here. |
In a recent post Kevin asks, in reference to a recurrent laryngeal nerve injury: Isn't part of informed consent acceptance of that risk? In some ways it is but it is not a shield from liability by any means. As one of his commenters put it:
Warning the patient of known complications of a procedure is protection against an informed consent lawsuit.Even more importantly informed consent is a process rather than simply a piece of paper. My office notes go into great detail about the risks, benefits and indications for a particular procedure and things that may increase that risk. If the patient described above had neck surgery or neck irraditaion in the past, that would increase the risks for nerve or parathyroid injury. Every procedure has a "buzzword" complication. Recurrent laryngeal nerve injury for thyroid surgery is one, common bile duct injury during laparoscopic cholecystectomy is another. Unless certain circumstances are in play, informed consent won't shield you from liability.
It is not an automatic protection or defense against lawsuit if the complication occurs. You still have to perform the procedure, and manage complications that might occur, provide adequate follow-up, etc, to the prevailing standard of care.
For example, you might warn me of bleeding. If I bleed to death, that doesn't protect you if it happened because you were negligent
Informed consent does provide some protection for common, "low impact" complications like wound infections. The infection rare from an uncomplicated appendectomy is about ten percent, but the treatment for it is simple. Since patients are made aware of this my liability exposure is low. Informed consent also allows for the unexpected. From the "boilerplate" consent form used in my office:
I understand that during the course of the procedure described above it may be necessary or appropriate to perform additional procedures which are unforeseen or not known to be needed at the time this consent is given. I consent to and authorize the performance of such additional procedures as they deem necessary or appropriate.
This allows for the treatment of the unexpected. Such as the colon malignancy found during exploratory laparotomy for trauma. Sometimes a colostomy has to be constructed when not expected. Under the statement above, as well as listing some circumstances as "special risks", you can be covered.
There is also the school of thought that informed consent cannot be completely given freely. They maintain that patients give consent under duress because if they do not give it, they will be denied surgery, so they will sign anything to relive their pain.
A discussion about informed consent may be found here. |
Thursday, April 14, 2005
Broken Hearts......
From The Wall Street Journal($$):For Some Transplant Patients,Diseased Hearts Are Lifesavers:
While the risks are many, some are willing to take them:
From The Wall Street Journal($$):For Some Transplant Patients,Diseased Hearts Are Lifesavers:
Every year about 500 people on the waiting list for a heart transplant die before an organ is made available. Thousands more die because they are considered too old or sick to get on the list to begin with.What a horrible waste of a scarce resource. But some centers are attempting to get some use from the "suboptimal heart":
But some heart surgeons are demonstrating that many of these people could be saved if transplant hospitals were less particular about the quality of donor hearts. They're starting programs that provide lower-quality hearts to older and sicker patients -- and sparking debate about how a transplant system that fails to help many people could be improved.
Beyond the 2,058 hearts transplanted last year, an additional 3,058 were offered by families of the newly dead, according to the nonprofit Scientific Registry of Transplant Recipients. But these hearts were rejected, often because they were not top quality. They were either buried or cremated with their original owners.
Hillel Laks, a transplant surgeon at the University of California at Los Angeles, contends that half the rejected hearts are suitable for transplanting. In his "alternate heart" program here, Dr. Laks refurbishes defective donor hearts, sometimes performing bypass surgery on their clogged arteries while the organs are on ice. He and his colleagues give infected donors heavy-duty antibiotics after brain death but before their hearts are removed. Sometimes, as in the case of Fred Austin, Dr. Laks simply puts an old heart in an old person.Here is how it works:
When Mr. Austin's failing heart brought him to the brink of death at age 75, he was too old to get one of the prime hearts used in mainstream transplant programs. UCLA offered him the heart of a 62-year-old donor -- one that other hospitals in the region didn't want.
Mr. Austin was delighted to get it. "I wouldn't have lasted another three months," he says. Eleven days after his surgery in December 2002, Mr. Austin called up some buddies for a game of golf. Now, at 77, he hits the links three times a week.
Mr. Austin, one of the oldest people ever to receive a transplant, was lucky. Some 50,000 people die each year of congestive heart failure, a progressive worsening of pumping function. Many of those patients would have liked to get placed on the heart-transplant waiting list but couldn't do so, doctors say.
The system for allocating hearts starts with a waiting list that gives priority to those who are sickest and have waited the longest. When a heart becomes available, the hospital treating the deceased person keeps him or her on life support and informs a regional "organ procurement organization." The organization, working through its waiting list, furiously makes calls to place the organ -- looking for a surgeon and patient, preferably nearby, who are ready to receive the heart right away.Even active infection doesn't get in the way:
With "marginal" hearts, the organization will often call around everywhere and find no takers. That's where UCLA and other hospitals with an "alternate" list come in. After everyone else says no, the organization will call one of these hospitals and look for an alternate patient to accept the marginal heart. Patients on the alternate list must agree that they won't ordinarily be eligible for a heart from the regular list.
The hearts that end up in alternate-list patients have various problems. A recent innovation at UCLA has been to accept hearts from patients who died from bacterial meningitis -- a practice viewed as almost unthinkable a few years ago. Over the past three years, nine such hearts have been transplanted at UCLA. Thanks to heavy antibiotic doses for both the donor and the recipient, none of the recipients have gotten meningitis so far.And the results are fairly comparable:
Duke, which established its alternate program in 2000, and Columbia, which began its program in 2001, both have found that alternate recipients do somewhat worse than standard ones but still fairly well. Columbia found that 75% to 80% of its alternate patients live a year after the transplant, combined with 90% in its regular program.Some don't think the "alternate list" is fair:
Doctors say that those who don't make it usually die from underlying health problems, not problems with the donated heart. "A lot of the hearts that we classified as marginal are working extremely well," says Donna M. Mancini, a cardiologist at Columbia University Medical Center.
Rather than setting up alternate lists, some centers believe the best policy is to expand their definition of who is eligible for the regular list. Many surgeons are now willing to put patients as old as 70 on the regular list, giving them the same chance as younger people to get a good-quality heart.So if you were an older patient in need of a heart transplant would you rather die on the waiting list for a heart from an eighteen year-old or take one from a 50 year old that you could get right away? I'll take the old one, thank you very much, since my other medical problems will likely do me in before the heart will give out. Are the oldsters being treated unfairly?
Cedars-Sinai Medical Center in Los Angeles dropped its alternate list several years ago on the theory that it wasn't fair. "If a patient is a candidate for transplantation he should get a good heart, and age should not be a discriminatory factor," says Alfredo Trento, director of cardiothoracic surgery.
UCLA's Dr. Laks sees it differently. Since top-quality hearts are "a scarce resource," Dr. Laks says, "we have an obligation to give the heart to someone who has the best chance of surviving."
While the risks are many, some are willing to take them:
That conclusion still leaves another ethical dilemma: How far should transplant centers go in using marginal organs? A handful of centers have tried transplanting hearts from patients with hepatitis C, a virus that can lead to fatal liver disease. UCLA suspended such transplants when several recipients were infected, though it may restart. At the Cleveland Clinic, the hepatitis C transplant program has been scaled back after a study found that 14% of recipients contracted severe liver disease.But the drive to make one's statistics look good, rather than ethics will limit the "alternate list":
But some desperate patients would rather live with hepatitis C than face imminent death. One 59-year-old accountant from Long Island, who asked that his name not be used, was assigned to the alternate list at New York-Presbyterian Hospital, the teaching hospital for Columbia University, because of diabetes and kidney trouble. In March 2002, he received a heart from a 45-year-old man infected with hepatitis C.
The recipient is at risk for contracting hepatitis, but he says he is grateful for the chance at life. "Three years ago I was a dead man, and now here I am," he says. "I feel fantastic. I have a job, I have a family, life is good."
Outside of big urban hospitals few people have access to alternate-heart programs -- in large part because surgeons fear risk-taking could harm their statistics. "Cardiac transplant programs all over the U.S. are carefully scrutinized for outcome. If programs fall below a certain standard, it's a big hassle because you have to justify your program to Medicare and insurance carriers," says James Kirkland, director of cardiothoracic transplants at the University of Alabama at Birmingham.(emphasis mine). So the cherry picking continues....
Partly for this reason, UAB doesn't have an alternate-heart program, but Dr. Kirkland is in the early stages of organizing an international clinical trial in which UAB would likely participate. The trial would compare the success of programs such as UCLA's to the implantation of a left ventricular assist device.
Labels: Transplantation
|Tuesday, April 12, 2005
Monday, April 11, 2005
Tales from the Trauma Service VIII...
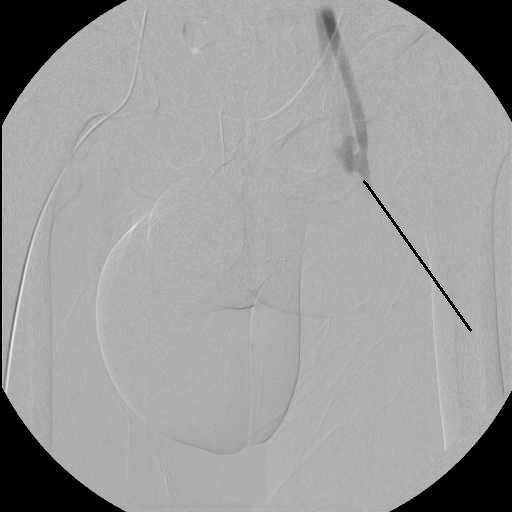
I seem to be collecting transaxial gunshot wounds lately. The latest is a 20-ish black man shot by a known assailant at an unknown range and with an unknown weapon. Hemodynamically stable but with an impressive physical exam finding I will show you in a moment. Initial AP pelvis film and urethrogram:

The yellow line points to the paperclip marking the entry wound. He had a 15 mm/HG difference in systolic pressure between his legs, with the right greater than the left. So I have to worry about a rectal, vascular, and genitourinary injury. Off to the angio suite we go:
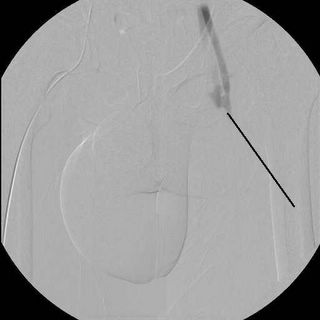
Looks like a pseudoaneursym, indicated by the black line, but wait....

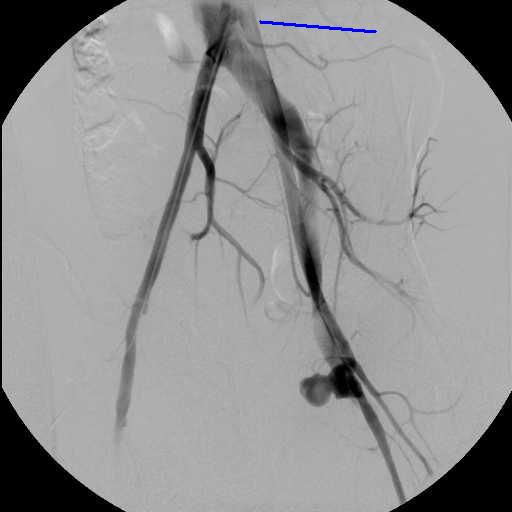
Rapid filling of the left femoral vein (blue line). Here is another view:

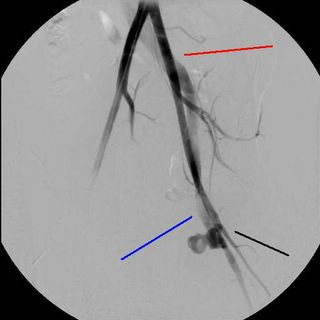
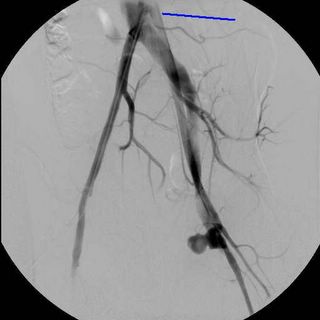
So he has a traumatic arterio-venous fistula from the superficial femoral artery and vein Options include endovascular stent-grafting or operative repair. Given his age, I opted for the latter. He went to the OR for a rigid sigmoidoscopy, which was negative, the urologist performed a cystoscopy and drainage for this injury. WARNING:NOT SAFE FOR WORK OR MANY OTHER PLACES.
The edema, first thought to be from a urethral injury, was hematoma from blood tracking along the wound tract. The vein had severe damage. Both were repaired primarily.
I seem to be collecting transaxial gunshot wounds lately. The latest is a 20-ish black man shot by a known assailant at an unknown range and with an unknown weapon. Hemodynamically stable but with an impressive physical exam finding I will show you in a moment. Initial AP pelvis film and urethrogram:

The yellow line points to the paperclip marking the entry wound. He had a 15 mm/HG difference in systolic pressure between his legs, with the right greater than the left. So I have to worry about a rectal, vascular, and genitourinary injury. Off to the angio suite we go:
Looks like a pseudoaneursym, indicated by the black line, but wait....

Rapid filling of the left femoral vein (blue line). Here is another view:


So he has a traumatic arterio-venous fistula from the superficial femoral artery and vein Options include endovascular stent-grafting or operative repair. Given his age, I opted for the latter. He went to the OR for a rigid sigmoidoscopy, which was negative, the urologist performed a cystoscopy and drainage for this injury. WARNING:NOT SAFE FOR WORK OR MANY OTHER PLACES.
The edema, first thought to be from a urethral injury, was hematoma from blood tracking along the wound tract. The vein had severe damage. Both were repaired primarily.
Labels: Tales from the Trauma Service
|Saturday, April 09, 2005
Wednesday, April 06, 2005
2005 Match Stats....
Mr. Genes, Grunt Doc, and Dr. Rack have analyzed the statistics from the 2005 Match. Here are some more numbers:
General Surgery had 1051 positions available this year (see page 4), up from 1044 last year. Of these 885 were filled by US applicants (80.3%) and 199 by non-US applicants (18.9%) for a total of 1044 applicants matching in general surgery (99%). Seven spots were unfilled. These numbers are slightly down from last year when US applicants filled about 85 percent of the slots, and only two slots were left unfilled. This represents the first decline in the number of US applicants matching in general surgery since 2002.
Family Practice had 2761 slots available this year, down from 2864 in 2004 and 2920 in 2003. 2275 slots were filled (82.4%), up from the 78.8 fill percentage last year. 1117 of the 2275 were filled by US seniors (49%), 1158 by non-US applicants (51%). The number of filled slots held by US applicants is down somewhat from 2004 when 52.5 percent of the filled slots were US applicants. The total fill percentage has ranged anywhere between 76-82 percent since 2001, while the total number of slots offered has fallen from 3074 in 2001 to 2761 this year. The percentage of filled slots held by US applicants has fallen from a high of 64 percent in 2001 as well.
Internal Medicine had 4634 slots filled out of the 4768 offered (97%). This is the same as last year and has been trending upward since 2001 (93%). Fifty-seven percent (2659) of those filled were filled by US applicants, up slightly from 56% last year. While the total number of offered slots has varied slightly from year to year, more slots were offered in 2005 compared to 2001 (4768 vs. 4727)
Pediatrics offered 2269 slots this year and filled 2211 of them (97.4%). The total number of slots were up slightly from 2004 (2261 vs. 2269) and the fill percentage was up by 1.7 percent as well. US applicants held 76% of the filled slots in 2005, up slightly from the 74.5 percent last year. This reverses a trend since 2001 when 81 percent of the filled slots were held by US applicants.
What does this mean? Is Family Practice in trouble? If FP offered the same number of slots as it did in 2001 (3074) their fill rate would have been 74% with only 36.3%of total slots held by US applicants. Can the availability of fellowships leading to high-paying specialist postitions explain how IM and Pediatrics outperform FP? I can see it more for IM, but I have no idea how much a pediatric pulmonologist or cardiologist makes compared with their adult colleagues.
One thing I thinks this makes abundantly clear, the solution to the primary care problem does not lie in providing more residency training slots, as they can't fill the ones they have even after reducing the numbers. |
Mr. Genes, Grunt Doc, and Dr. Rack have analyzed the statistics from the 2005 Match. Here are some more numbers:
General Surgery had 1051 positions available this year (see page 4), up from 1044 last year. Of these 885 were filled by US applicants (80.3%) and 199 by non-US applicants (18.9%) for a total of 1044 applicants matching in general surgery (99%). Seven spots were unfilled. These numbers are slightly down from last year when US applicants filled about 85 percent of the slots, and only two slots were left unfilled. This represents the first decline in the number of US applicants matching in general surgery since 2002.
Family Practice had 2761 slots available this year, down from 2864 in 2004 and 2920 in 2003. 2275 slots were filled (82.4%), up from the 78.8 fill percentage last year. 1117 of the 2275 were filled by US seniors (49%), 1158 by non-US applicants (51%). The number of filled slots held by US applicants is down somewhat from 2004 when 52.5 percent of the filled slots were US applicants. The total fill percentage has ranged anywhere between 76-82 percent since 2001, while the total number of slots offered has fallen from 3074 in 2001 to 2761 this year. The percentage of filled slots held by US applicants has fallen from a high of 64 percent in 2001 as well.
Internal Medicine had 4634 slots filled out of the 4768 offered (97%). This is the same as last year and has been trending upward since 2001 (93%). Fifty-seven percent (2659) of those filled were filled by US applicants, up slightly from 56% last year. While the total number of offered slots has varied slightly from year to year, more slots were offered in 2005 compared to 2001 (4768 vs. 4727)
Pediatrics offered 2269 slots this year and filled 2211 of them (97.4%). The total number of slots were up slightly from 2004 (2261 vs. 2269) and the fill percentage was up by 1.7 percent as well. US applicants held 76% of the filled slots in 2005, up slightly from the 74.5 percent last year. This reverses a trend since 2001 when 81 percent of the filled slots were held by US applicants.
What does this mean? Is Family Practice in trouble? If FP offered the same number of slots as it did in 2001 (3074) their fill rate would have been 74% with only 36.3%of total slots held by US applicants. Can the availability of fellowships leading to high-paying specialist postitions explain how IM and Pediatrics outperform FP? I can see it more for IM, but I have no idea how much a pediatric pulmonologist or cardiologist makes compared with their adult colleagues.
One thing I thinks this makes abundantly clear, the solution to the primary care problem does not lie in providing more residency training slots, as they can't fill the ones they have even after reducing the numbers. |
Tuesday, April 05, 2005
The Medical Marketplace....
From The Wall Street Journal($$):Childbirth for Bargain-Hunters:
So when patients treat the payment for medical services like buying a car they are praised for their spunk and inventiveness. But when hospitals and physicians bring up the economic angle they are denounced as scoundrels.
What a system like the one above will do may not necessarily lower costs, but would certainly allow you to get your money's worth. If I have less complications and better outcomes from a procedure than the surgeon down the street you better believe that I will charge more. Of course feel free to face a wound infection rate twice as high as mine or a one in ten chance of a common bile duct injury and pay 75% of my fee, but remember caveat emptor.
This could also lead to cost shifting according to patient risk. Right now I am paid the same for a cholecsytectomy performed on a healthy 25 year-old as well as a diabetic 70 year-old who smokes and has had three AMI's. In the open air medical flea market I could offer a sliding scale with a "smoking surcharge", "diabetic surcharge", "non-compliance surcharge",ect.....Sound fair to you? Depends on where you would fit on the fee schedule most likely.
To be fair the marketplace would have to work in both directions. Given what I have seen so far, I don't think it would. |
From The Wall Street Journal($$):Childbirth for Bargain-Hunters:
Expecting her third child this winter, Sandra Hughes became an unexpected pioneer in the new world of health care -- a world in which consumers have a direct stake in limiting their spending on treatment and tests.And shop around they will:
Mrs. Hughes and her self-employed husband had health insurance, but couldn't get maternity coverage because of two previous Caesareans. So in nine months, Mrs. Hughes went from novice health-care consumer to hard-knuckled haggler. She negotiated discounts with doctors, convinced her obstetrician to match another's offer and wrote to the chief executive of a local hospital demanding a reason for refusing to meet her price.
"In the beginning, you think, wait, this is my health care: I don't want to make these people mad or insult them by talking money," says the 31-year-old former special-education teacher. "But after a while, it felt like I was buying a car."
Pregnant women are by necessity and ingenuity paving the way in what is called "consumer driven" health care. As companies boost premiums for family coverage -- and in some cases drop dependents altogether -- a growing group of women lack health coverage for pregnancy, one of the biggest medical costs they face. Others are in some type of consumer-driven high-deductible plan, with a Health Savings Account, that gives patients incentives to shop around.
Ronna Alexander, a self-employed design consultant in Douglas, Mich., had a medical savings account and catastrophic-care policy, so she and her husband were used to paying upfront for much of their health care.What if the home birth goes wrong? Does the "break glass in case of emergency" OB/GYN get a cut of the $2200?
When she called hospitals for maternity-related prices, they were reluctant to break down specific charges, arguing that every delivery is different. By her 20th week, she says she already had paid out about $800 in prenatal care, but felt that most of the tests were done to protect her doctors against liability and that they had little time for counseling -- a sense all the more acute because she was paying the bills. So she made an appointment with a midwife who does only home births, even though "I am the last person who would do a home birth."
She liked the midwife's more-attentive approach, and the price: only $1,800. Yolanda Visser of Grand Rapids, the certified professional midwife, says that for about half of the mothers she works with, price is at least one factor in having a home birth. She now charges $2,200 for full prenatal care and delivery.
The new focus on limiting costs is putting added pressure on expectant parents. When Deborah Elissagaray and her husband shopped for a family policy a couple of years ago, they felt they couldn't afford an extra $200 to $300 for maternity coverage on top of the $700 a month for regular medical insurance. The couple was just starting up a winery in Placerville, Calif. Their broker assured that if they did have a child, they would spend less money by paying for it themselves.And....
When Mrs. Elissagaray became pregnant about six months later, she and her husband thought they would have to rely on money from their 401(k)s and part of a business loan. Worse, she says, was having to decide whether to forgo some prenatal tests, including a $3,000 amniocentesis test for genetic diseases. At age 38, she was at higher risk for having a baby with problems such as Down syndrome. She went ahead with the test.
In the end, Mrs. Elissagaray wound up qualifying for a maternity-assistance program in California called AIM, targeted at people who aren't poor enough to qualify for Medicaid. "When I found out, I cried right there in the office," she says. Her baby, Olivia, was born in February.
When Sandra Hughes in Florida reviewed a breakdown of what her previous insurer paid for her last pregnancy it showed her the rates were much lower than what the doctors and hospital charged so-called cash patients who pay out of pocket. When she asked for the same deal on her current pregnancy, one obstetrician complied. When she asked another doctor's practice to match it they did, cutting the usual $3,000 fee to $1,900.
When she tried the same with the hospital, she met resistance. Although her old insurer had paid $3,200 for her last Caesarean section there, Mease Dunedin Hospital in Dunedin, Fla., said its best price for a cash patient was $5,000. She says she wrote Jim Pfeiffer, president and chief executive of Mease Hospitals, demanding he justify the discrepancy. "By then, I was almost nine months pregnant, and I was angry!" she says.
Mr. Pfeiffer says he didn't receive the letter, but says the hospital's average cost for a Caesarean is actually $5,100, with a list price of about $10,200.
Since she already had negotiated deals with an anesthesiologist at Mease Dunedin and liked the care there before, she choose to remain at the hospital. But she says, "If more people asked about prices, it would all be far more transparent."
So when patients treat the payment for medical services like buying a car they are praised for their spunk and inventiveness. But when hospitals and physicians bring up the economic angle they are denounced as scoundrels.
What a system like the one above will do may not necessarily lower costs, but would certainly allow you to get your money's worth. If I have less complications and better outcomes from a procedure than the surgeon down the street you better believe that I will charge more. Of course feel free to face a wound infection rate twice as high as mine or a one in ten chance of a common bile duct injury and pay 75% of my fee, but remember caveat emptor.
This could also lead to cost shifting according to patient risk. Right now I am paid the same for a cholecsytectomy performed on a healthy 25 year-old as well as a diabetic 70 year-old who smokes and has had three AMI's. In the open air medical flea market I could offer a sliding scale with a "smoking surcharge", "diabetic surcharge", "non-compliance surcharge",ect.....Sound fair to you? Depends on where you would fit on the fee schedule most likely.
To be fair the marketplace would have to work in both directions. Given what I have seen so far, I don't think it would. |
Grand Rounds XXVIII....
Hosted by Polite Dissent and as a bonus it is approved:

For your protection. |
Hosted by Polite Dissent and as a bonus it is approved:
For your protection. |
Monday, April 04, 2005
Specialists versus Primary Care....
From American Medical News:Work force study tackles specialty vs. primary care
Haven't we heard this before? Weren't we told years ago that there were too many specialists? Has anything changed?
Some disagree with the study and point out some flaws:
For good or ill, patients belive that specialists deliver better care. In the medicine side of the house that is subject to debate. But in the proceduralist wing research shows that more of a procedure you do (i.e. specialize in doing something)the better outcomes you have. (See the "Practice Makes Perfect" posts to the right).
Mr Holt opines here. |
From American Medical News:Work force study tackles specialty vs. primary care
As policy-makers and medical community leaders determine the best response to physician shortage predictions, the question of whether the public will need more primary care physicians or more specialists is back on the table.
Work force experts and organized medicine leaders remain divided on how to answer that. And with no national health policy to guide medical school expansion, state legislators and medical educators likely will follow the discussions closely.
The latest salvo in the debate comes from Barbara Starfield, MD, MPH, with the Johns Hopkins School of Public Health. Her study's conclusion: The greater the supply of primary care physicians, the lower the mortality rate. She also found that a higher specialist-to-population ratio did not decrease mortality rates. In fact, she determined that too many specialists negatively impacts communities because patients are more likely to have unnecessary tests and procedures.
The nationwide study, "The Effects of Specialist Supply on Populations' Health: Assessing the Evidence," released in a Web-only March 15 edition of Health Affairs looked at mortality rates at the county level.
"Decisions about the physician supply should be made on the basis of evidence for their utility in improving health and reducing ill health and deaths," Dr. Starfield said. "Currently, the United States has many more specialists than do other comparable countries with better health levels."
Robert L. Phillips Jr., MD, MSPH, director of the Robert Graham Center, supported the study in his own commentary in Health Affairs.
"If we want our health care system to be an economic engine, we are headed in the right direction," Dr. Phillips said in an interview. "If what we want is a healthier population, we are headed in the wrong direction."
Specialists aren't bad, he said, but if the physician work force is going to expand, there is an opportunity to ask how it should be configured to make Americans healthier.
"Increasing the supply of subspecialists is not the way to go," he said. "This is not an indictment, but we have an option here, and physicians should weigh in on what's important to them."
Haven't we heard this before? Weren't we told years ago that there were too many specialists? Has anything changed?
Some disagree with the study and point out some flaws:
In his critique, also published in Health Affairs, Salsberg questioned the validity of looking at the number of specialists by county and linking that to mortality rates.
Specialists, Salsberg said, tend to concentrate in urban areas that draw patients from large geographical areas, so they can see enough cases to be clinically sharp and financially viable. At the same time, the population that dominates urban areas tends to be higher risk and has higher mortality rates.
An analysis of mortality rates also does not capture quality-of-life improvements that specialists provide, he said. Ophthalmologists might not save lives, but cataract surgery can make the difference in a person's ability to see to drive or read.
In addition, he argued, many scientific advances have come from greater specialization. Achievements might mean drugs or treatments that primary care physicians can provide for patients, but they also result in highly complex treatments best handled by the subspecialists themselves, he said.
For good or ill, patients belive that specialists deliver better care. In the medicine side of the house that is subject to debate. But in the proceduralist wing research shows that more of a procedure you do (i.e. specialize in doing something)the better outcomes you have. (See the "Practice Makes Perfect" posts to the right).
Mr Holt opines here. |
![]()





