Saturday, July 15, 2006
Another Surgeon Joins the Fold.....
Thanks to Orac for the heads-up. Sid Schwab, who's book I reviewed here, has started a blog: Surgeonsblog. |
Thanks to Orac for the heads-up. Sid Schwab, who's book I reviewed here, has started a blog: Surgeonsblog. |
Friday, July 14, 2006
Priorities.....
A patient struck by a hit-and-run driver. Severe head injury. Being young and otherwise healthy the patient did not carry any health insurance. The patient has been ready for discharge to rehab now for over two weeks, but funding is an issue. The patient was active in the local music "scene" and their friends have put on several fundraisers to assist in costs. This prompted the following letter to the editor of the local paper:
Given the quality of the local paper, probably not. But it is a worthy point to make just the same. |
A patient struck by a hit-and-run driver. Severe head injury. Being young and otherwise healthy the patient did not carry any health insurance. The patient has been ready for discharge to rehab now for over two weeks, but funding is an issue. The patient was active in the local music "scene" and their friends have put on several fundraisers to assist in costs. This prompted the following letter to the editor of the local paper:
I read with interest about the generous outpouring of support for Xxxx Yyyy, seriously injured by a hit-and-run driver. The Yyyy family has had much to deal with, and planning for Xxxx's rehabilitation is certainly helped by the fund-raising efforts of friends. But what about the group that struggled against tremendous odds to bring them back from the brink of death?
I am the neurosurgeon who treated Xxxx as they arrived at the Big Hospital's Emergency-Trauma Center. Had it not been for the rapid response of the trauma team, the doctors, nurses and staff of the Emergency Trauma Center, the surgical ICU and Neuro Nursing Unit, the story would have had another ending.
It was not luck that those resources are available. It is a program that has been supported and developed over many years of commitment by Big Hospital, a cadre of local private physicians and a dedicated team of professionals that assures every person in our area will be given a fighting chance should they be traumatically injured.
It seems just a bit ironic that the focus of the community is now is on raising money for a hospitalization at a financially well-endowed facility that will not admit Xxxx until all the cost of their treatment is paid, up front, while the many physician specialists, nurses and clinical professionals who actually saved their life are likely not to be paid at all.
The people and the organization that saved the Yyyy family from planning a funeral have not been fully recognized. There is a discussion begging to be had concerning the large number of uninsured people in our country, and the dangerous erosion of the safety net that trauma centers and community hospitals provide. Perhaps Xxxx's story will stimulate your paper to lead that discussion.
Given the quality of the local paper, probably not. But it is a worthy point to make just the same. |
Thursday, July 13, 2006
Tales From the Operating Room X.....
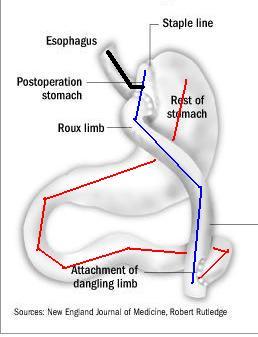
Or when gastric bypass is not your friend. Young patient several years out from laparoscopic gastric bypass presents with severe abdominal pain. Over the past several weeks they have had intermittent attacks of pain which lasted only a few minutes. This episode did not resolve and they were diagnosed with a small bowel obstruction. The patient underwent nasogastric decompression, a not too effective maneuver as you see here:
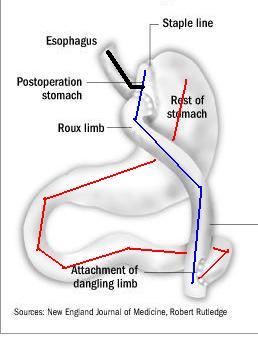
The black line represents the NG tube. With the majority of the stomach and small bowel excluded (red) the only area that can be decompressed is seen in blue. A few hours later the patient developed hypotension and I was called to evaluate the patient. They had guarding and rebound on abdominal examination. Off to the OR. Gross pictures follow.
[
[
[
[
[
[
[
[
[
[
[
[
[

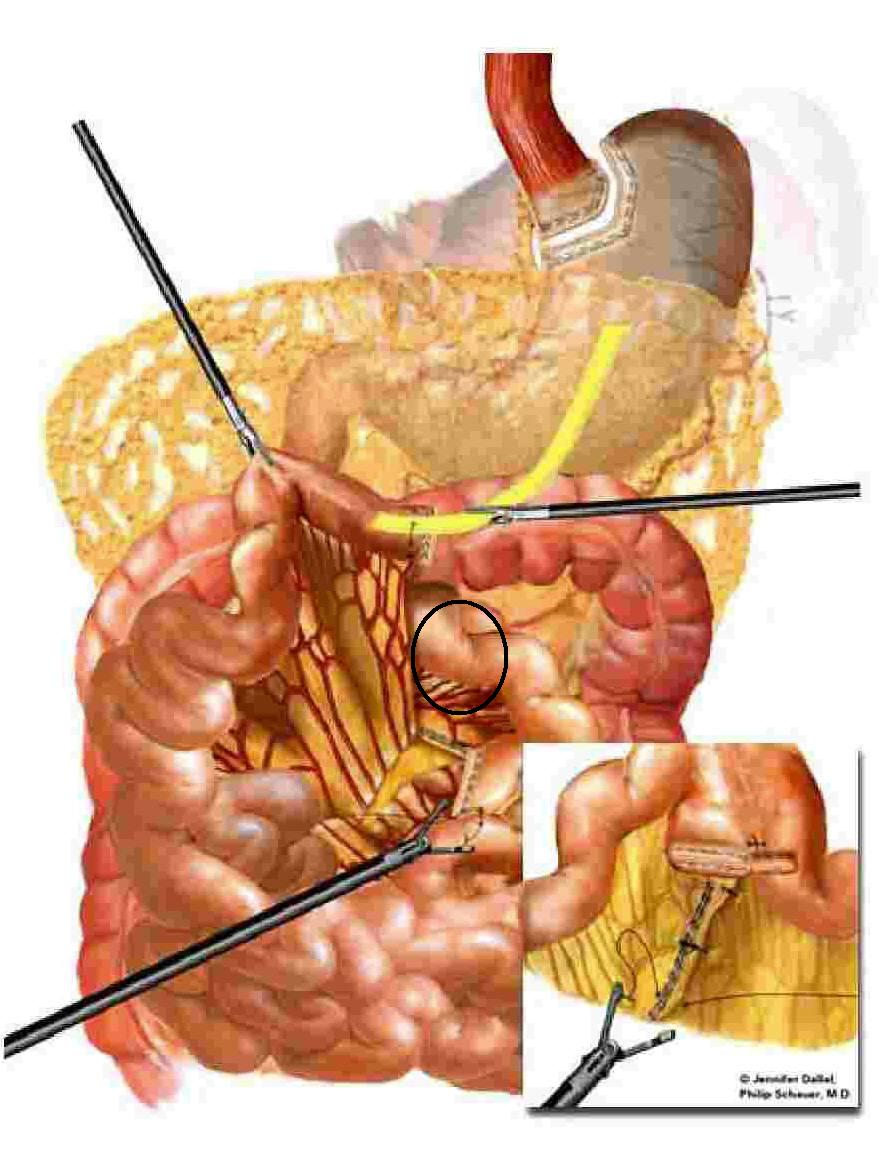
The yellow circle represents the jejunal anastamosis. Here is another view.

The yellow circle indicates the transverse colon. Obviously this bowel is severely ischemic. The vast majority of the small bowel will need to be removed. How did it become so? It was due to an internal hernia posterior to the bypass limb. The area in question is indicated by the black circle.

The hernia was reduced and the bowel irrigated with warm saline, we spoke softly to it and used flourescin and a Woods lamp, but to no avail. The small bowel from the ligament of Treitz to the terminal ileum was removed. About a third of the roux limb was also removed. By my crude measurements this left about 50 cm of small bowel en vivo. The cecum was marginal but the length of small bowel needed is reduced if the ileocecal valve is intact. A gastrostomy and duodenostomy were placed to allow for decompression.
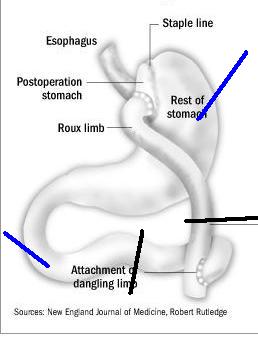
The black lines represent the resection lines and the blue lines represent the locations of the tubes. The patient was acidotic and hypothermic so the procedure was abandoned to allow for resuscitation in the ICU and a second look in 24 hours.
They required all sorts of blood products but by morning the patient was out of shock and ready for the return trip.
Which was disappointing.
The marginal terminal ileum and cecum were necrotic, as was another third of the roux limb. This left them with about 25-30 cm of small bowel. The end of the roux limb was exteriorized as an ostomy.
The patient recovered and shortly before discharge I placed a port for TPN. I saw the patient back in the office the other day and they are doing as well as can be expected. Now we have to send them off for additional surgery to restore continuity of the bowel.
Oh, and since this was a complication from a non-covered procedure, their insurance is not paying for any of this. Not the hospital, not my fees, not the home TPN. |
Or when gastric bypass is not your friend. Young patient several years out from laparoscopic gastric bypass presents with severe abdominal pain. Over the past several weeks they have had intermittent attacks of pain which lasted only a few minutes. This episode did not resolve and they were diagnosed with a small bowel obstruction. The patient underwent nasogastric decompression, a not too effective maneuver as you see here:
The black line represents the NG tube. With the majority of the stomach and small bowel excluded (red) the only area that can be decompressed is seen in blue. A few hours later the patient developed hypotension and I was called to evaluate the patient. They had guarding and rebound on abdominal examination. Off to the OR. Gross pictures follow.
[
[
[
[
[
[
[
[
[
[
[
[
[

The yellow circle represents the jejunal anastamosis. Here is another view.

The yellow circle indicates the transverse colon. Obviously this bowel is severely ischemic. The vast majority of the small bowel will need to be removed. How did it become so? It was due to an internal hernia posterior to the bypass limb. The area in question is indicated by the black circle.
The hernia was reduced and the bowel irrigated with warm saline, we spoke softly to it and used flourescin and a Woods lamp, but to no avail. The small bowel from the ligament of Treitz to the terminal ileum was removed. About a third of the roux limb was also removed. By my crude measurements this left about 50 cm of small bowel en vivo. The cecum was marginal but the length of small bowel needed is reduced if the ileocecal valve is intact. A gastrostomy and duodenostomy were placed to allow for decompression.

The black lines represent the resection lines and the blue lines represent the locations of the tubes. The patient was acidotic and hypothermic so the procedure was abandoned to allow for resuscitation in the ICU and a second look in 24 hours.
They required all sorts of blood products but by morning the patient was out of shock and ready for the return trip.
Which was disappointing.
The marginal terminal ileum and cecum were necrotic, as was another third of the roux limb. This left them with about 25-30 cm of small bowel. The end of the roux limb was exteriorized as an ostomy.
The patient recovered and shortly before discharge I placed a port for TPN. I saw the patient back in the office the other day and they are doing as well as can be expected. Now we have to send them off for additional surgery to restore continuity of the bowel.
Oh, and since this was a complication from a non-covered procedure, their insurance is not paying for any of this. Not the hospital, not my fees, not the home TPN. |
Friday, July 07, 2006
Books for the Young Surgeon....
As the 1,046 new surgical interns start their residency locations some of them may be curious about what books they should buy. Many probably have some already, others may not have anything except the book from their third-year clerkship. The factor that will determine the size of your library more than anything is the size of your educational stipend. Some suggestions follow, the titles in italics are those I currently own, even in an older edition:
You will need a "all around" surgical textbook. The "big three" are Sabiston's Textbook of Surgery, Schwartz's Principles of Surgery, and Greenfield's Surgery: Scientific Principles and Practice . I primarily used the Greenfield book as a resident, and just purchased the fourth edition. Get one with a CD ROM or online updates. Since you only have six months before your first inservice exam quick review will be necessary. Either Essentials of General Surgery or Advanced Surgical Recall should suffice.
Other books you may find useful along the way:
With the emphasis on basic science, a basic science for surgeons book may be helpful. I used O'Leary's The Physiologic Basis of Surgery when I was a resident. A new edition of Basic Science Review for Surgeons is coming out in the fall.
As you move "up the food chain" these purchases my be helpful. You will need a surgical atlas, Zollinger's Atlas of Surgical Operations is the most popular. Also very useful is Cameron's Current Surgical Therapy . Other upper level general surgery books that I have found helpful have been; Mastery of Surgery and Maingot's Abdominal Operations (although in need of an update). Although not a book, a subscription to Selected Readings in General Surgery provides commentary on what's out there in the surgical literature.
Some specialty books you might like to have include:
Trauma and its accompanying handbook, the Trauma Manual. Another great trauma book is Top Knife: The Art & Craft in Trauma Surgery.
For more expansive coverage of critical care there are new editions of Shoemaker's Textbook of Critical Care as well as Civetta's Critical Care . Lighter, but still helpful, is the The ICU Book, with a new edition coming out this September.
For your vascular experience there is the massive Vascular Surgery by Rutherford and the smaller Current Therapy in Vascular Surgery.
Other books I found helpful were Ashcraft's Pediatric Surgery, Principles and Practices of Surgery for the Colon, Rectum and Anus, and if your book fund is really generous, The Breast : Comprehensive Management of Benign and Malignant Disorders.
And also, while not a book, the latest edition of SESAP provides many questions and answers.
I hope the list has been helpful. Enjoy your reading! |
As the 1,046 new surgical interns start their residency locations some of them may be curious about what books they should buy. Many probably have some already, others may not have anything except the book from their third-year clerkship. The factor that will determine the size of your library more than anything is the size of your educational stipend. Some suggestions follow, the titles in italics are those I currently own, even in an older edition:
You will need a "all around" surgical textbook. The "big three" are Sabiston's Textbook of Surgery, Schwartz's Principles of Surgery, and Greenfield's Surgery: Scientific Principles and Practice . I primarily used the Greenfield book as a resident, and just purchased the fourth edition. Get one with a CD ROM or online updates. Since you only have six months before your first inservice exam quick review will be necessary. Either Essentials of General Surgery or Advanced Surgical Recall should suffice.
Other books you may find useful along the way:
With the emphasis on basic science, a basic science for surgeons book may be helpful. I used O'Leary's The Physiologic Basis of Surgery when I was a resident. A new edition of Basic Science Review for Surgeons is coming out in the fall.
As you move "up the food chain" these purchases my be helpful. You will need a surgical atlas, Zollinger's Atlas of Surgical Operations is the most popular. Also very useful is Cameron's Current Surgical Therapy . Other upper level general surgery books that I have found helpful have been; Mastery of Surgery and Maingot's Abdominal Operations (although in need of an update). Although not a book, a subscription to Selected Readings in General Surgery provides commentary on what's out there in the surgical literature.
Some specialty books you might like to have include:
Trauma and its accompanying handbook, the Trauma Manual. Another great trauma book is Top Knife: The Art & Craft in Trauma Surgery.
For more expansive coverage of critical care there are new editions of Shoemaker's Textbook of Critical Care as well as Civetta's Critical Care . Lighter, but still helpful, is the The ICU Book, with a new edition coming out this September.
For your vascular experience there is the massive Vascular Surgery by Rutherford and the smaller Current Therapy in Vascular Surgery.
Other books I found helpful were Ashcraft's Pediatric Surgery, Principles and Practices of Surgery for the Colon, Rectum and Anus, and if your book fund is really generous, The Breast : Comprehensive Management of Benign and Malignant Disorders.
And also, while not a book, the latest edition of SESAP provides many questions and answers.
I hope the list has been helpful. Enjoy your reading! |
Thursday, July 06, 2006
Advice for the New Doctor......
I first posted this two years ago, but it bears repeating:
Sew well, cut well, get well.
If in doubt, put in a drain.
If in doubt, use retention sutures.
It is better to have it and not need it than to need it and not have it.
You can't go wrong by getting out of bed.
Turn the PEEP down before sticking for a central line.
Honesty is the coin of the realm NEVER, EVER LIE
Make sure you read. With the new workhour limits your in-hospital education time is reduced. You need to read outside of the hospital. Every day.
If storms are ahead, load the boat.
Eat when you can, sleep when you can, and go to the bathroom when you can.
If it is not written in the chart, it did not happen.
"No truer friend, no worse enemy" applies not only to the Marine Corps but to the nursing staff as well. Treat nurses, respiratory therapists, phlebotomists, scrub techs, and all hospital personnel with respect. They can hurt you worse.
Better is the enemy of good.
Never prep yourself out of a good operation.
For the most part, all of the good operations have been invented, but there is always room for variations on a theme.
Never be the first, or the last, to perform a procedure, or prescribe a treatment.
The only thing more dangerous than an intern with a new pen is a resident with a new paper.
They can beat you down, but they can't stop the clock. |
I first posted this two years ago, but it bears repeating:
Sew well, cut well, get well.
If in doubt, put in a drain.
If in doubt, use retention sutures.
It is better to have it and not need it than to need it and not have it.
You can't go wrong by getting out of bed.
Turn the PEEP down before sticking for a central line.
Honesty is the coin of the realm NEVER, EVER LIE
Make sure you read. With the new workhour limits your in-hospital education time is reduced. You need to read outside of the hospital. Every day.
If storms are ahead, load the boat.
Eat when you can, sleep when you can, and go to the bathroom when you can.
If it is not written in the chart, it did not happen.
"No truer friend, no worse enemy" applies not only to the Marine Corps but to the nursing staff as well. Treat nurses, respiratory therapists, phlebotomists, scrub techs, and all hospital personnel with respect. They can hurt you worse.
Better is the enemy of good.
Never prep yourself out of a good operation.
For the most part, all of the good operations have been invented, but there is always room for variations on a theme.
Never be the first, or the last, to perform a procedure, or prescribe a treatment.
The only thing more dangerous than an intern with a new pen is a resident with a new paper.
They can beat you down, but they can't stop the clock. |
Belated Birthday Post.....
Everyone seemed to be smoking pot, drinking, and wrecking their cars this past weekend, so I was unable to put up my planned post. The medical blogosphere has grown by leaps and bounds over the past three years. One only needs to look at the submissions and hosts for Grand Rounds to see that. There is also now "spawn of Grand Rounds" with Radiology Grand Rounds and the "Cheese Wheel" of literary medical bloggers.
But others have decided to hang it up. Galen has moved on, Dr. Wigton appears to have taken Red State Moron down, Geeknurse had to quit blogging due to job pressures, and Shrinkette has folded up her couch. I'm sure many others have passed on recently as well, but with so many new ones it has become nearly impossible to keep up. The biggest loss, of course, was the decision of my (and likely yours as well) blogmother to retire. Dr. Smith cited lack of time and her desire not to put out a substandard product as her main motivators to cease blogging. My time is becoming more compressed as well, especially with the planned fellowship sabbatical coming up in less than a year. I won't quit just yet. I have less concerns about quality writing, since I write mostly crap anyway, and I always can count on new and exciting Tales from The Trauma Service/Operating Room to keep posts going. No I won't quit, but I think I'll stick with the free Blogger for now. |
Everyone seemed to be smoking pot, drinking, and wrecking their cars this past weekend, so I was unable to put up my planned post. The medical blogosphere has grown by leaps and bounds over the past three years. One only needs to look at the submissions and hosts for Grand Rounds to see that. There is also now "spawn of Grand Rounds" with Radiology Grand Rounds and the "Cheese Wheel" of literary medical bloggers.
But others have decided to hang it up. Galen has moved on, Dr. Wigton appears to have taken Red State Moron down, Geeknurse had to quit blogging due to job pressures, and Shrinkette has folded up her couch. I'm sure many others have passed on recently as well, but with so many new ones it has become nearly impossible to keep up. The biggest loss, of course, was the decision of my (and likely yours as well) blogmother to retire. Dr. Smith cited lack of time and her desire not to put out a substandard product as her main motivators to cease blogging. My time is becoming more compressed as well, especially with the planned fellowship sabbatical coming up in less than a year. I won't quit just yet. I have less concerns about quality writing, since I write mostly crap anyway, and I always can count on new and exciting Tales from The Trauma Service/Operating Room to keep posts going. No I won't quit, but I think I'll stick with the free Blogger for now. |
Tuesday, July 04, 2006
Two-Hundred-Thirty Years Ago...
IN CONGRESS, July 4, 1776.
The unanimous Declaration of the thirteen united States of America,
When in the Course of human events, it becomes necessary for one people to dissolve the political bands which have connected them with another, and to assume among the powers of the earth, the separate and equal station to which the Laws of Nature and of Nature's God entitle them, a decent respect to the opinions of mankind requires that they should declare the causes which impel them to the separation.
We hold these truths to be self-evident, that all men are created equal, that they are endowed by their Creator with certain unalienable Rights, that among these are Life, Liberty and the pursuit of Happiness.--That to secure these rights, Governments are instituted among Men, deriving their just powers from the consent of the governed, --That whenever any Form of Government becomes destructive of these ends, it is the Right of the People to alter or to abolish it, and to institute new Government, laying its foundation on such principles and organizing its powers in such form, as to them shall seem most likely to effect their Safety and Happiness. Prudence, indeed, will dictate that Governments long established should not be changed for light and transient causes; and accordingly all experience hath shewn, that mankind are more disposed to suffer, while evils are sufferable, than to right themselves by abolishing the forms to which they are accustomed. But when a long train of abuses and usurpations, pursuing invariably the same Object evinces a design to reduce them under absolute Despotism, it is their right, it is their duty, to throw off such Government, and to provide new Guards for their future security.--Such has been the patient sufferance of these Colonies; and such is now the necessity which constrains them to alter their former Systems of Government. The history of the present King of Great Britain is a history of repeated injuries and usurpations, all having in direct object the establishment of an absolute Tyranny over these States. To prove this, let Facts be submitted to a candid world.
He has refused his Assent to Laws, the most wholesome and necessary for the public good.
He has forbidden his Governors to pass Laws of immediate and pressing importance, unless suspended in their operation till his Assent should be obtained; and when so suspended, he has utterly neglected to attend to them.
He has refused to pass other Laws for the accommodation of large districts of people, unless those people would relinquish the right of Representation in the Legislature, a right inestimable to them and formidable to tyrants only.
He has called together legislative bodies at places unusual, uncomfortable, and distant from the depository of their public Records, for the sole purpose of fatiguing them into compliance with his measures.
He has dissolved Representative Houses repeatedly, for opposing with manly firmness his invasions on the rights of the people.
He has refused for a long time, after such dissolutions, to cause others to be elected; whereby the Legislative powers, incapable of Annihilation, have returned to the People at large for their exercise; the State remaining in the mean time exposed to all the dangers of invasion from without, and convulsions within.
He has endeavoured to prevent the population of these States; for that purpose obstructing the Laws for Naturalization of Foreigners; refusing to pass others to encourage their migrations hither, and raising the conditions of new Appropriations of Lands.
He has obstructed the Administration of Justice, by refusing his Assent to Laws for establishing Judiciary powers.
He has made Judges dependent on his Will alone, for the tenure of their offices, and the amount and payment of their salaries.
He has erected a multitude of New Offices, and sent hither swarms of Officers to harrass our people, and eat out their substance.
He has kept among us, in times of peace, Standing Armies without the Consent of our legislatures.
He has affected to render the Military independent of and superior to the Civil power.
He has combined with others to subject us to a jurisdiction foreign to our constitution, and unacknowledged by our laws; giving his Assent to their Acts of pretended Legislation:
For Quartering large bodies of armed troops among us:
For protecting them, by a mock Trial, from punishment for any Murders which they should commit on the Inhabitants of these States:
For cutting off our Trade with all parts of the world:
For imposing Taxes on us without our Consent:
For depriving us in many cases, of the benefits of Trial by Jury:
For transporting us beyond Seas to be tried for pretended offences
For abolishing the free System of English Laws in a neighbouring Province, establishing therein an Arbitrary government, and enlarging its Boundaries so as to render it at once an example and fit instrument for introducing the same absolute rule into these Colonies:
For taking away our Charters, abolishing our most valuable Laws, and altering fundamentally the Forms of our Governments:
For suspending our own Legislatures, and declaring themselves invested with power to legislate for us in all cases whatsoever.
He has abdicated Government here, by declaring us out of his Protection and waging War against us.
He has plundered our seas, ravaged our Coasts, burnt our towns, and destroyed the lives of our people.
He is at this time transporting large Armies of foreign Mercenaries to compleat the works of death, desolation and tyranny, already begun with circumstances of Cruelty & perfidy scarcely paralleled in the most barbarous ages, and totally unworthy the Head of a civilized nation.
He has constrained our fellow Citizens taken Captive on the high Seas to bear Arms against their Country, to become the executioners of their friends and Brethren, or to fall themselves by their Hands.
He has excited domestic insurrections amongst us, and has endeavoured to bring on the inhabitants of our frontiers, the merciless Indian Savages, whose known rule of warfare, is an undistinguished destruction of all ages, sexes and conditions.
In every stage of these Oppressions We have Petitioned for Redress in the most humble terms: Our repeated Petitions have been answered only by repeated injury. A Prince whose character is thus marked by every act which may define a Tyrant, is unfit to be the ruler of a free people.
Nor have We been wanting in attentions to our Brittish brethren. We have warned them from time to time of attempts by their legislature to extend an unwarrantable jurisdiction over us. We have reminded them of the circumstances of our emigration and settlement here. We have appealed to their native justice and magnanimity, and we have conjured them by the ties of our common kindred to disavow these usurpations, which, would inevitably interrupt our connections and correspondence. They too have been deaf to the voice of justice and of consanguinity. We must, therefore, acquiesce in the necessity, which denounces our Separation, and hold them, as we hold the rest of mankind, Enemies in War, in Peace Friends.
We, therefore, the Representatives of the united States of America, in General Congress, Assembled, appealing to the Supreme Judge of the world for the rectitude of our intentions, do, in the Name, and by Authority of the good People of these Colonies, solemnly publish and declare, That these United Colonies are, and of Right ought to be Free and Independent States; that they are Absolved from all Allegiance to the British Crown, and that all political connection between them and the State of Great Britain, is and ought to be totally dissolved; and that as Free and Independent States, they have full Power to levy War, conclude Peace, contract Alliances, establish Commerce, and to do all other Acts and Things which Independent States may of right do. And for the support of this Declaration, with a firm reliance on the protection of divine Providence, we mutually pledge to each other our Lives, our Fortunes and our sacred Honor. |
Now We Are Three.....
Too bad I had the On Call Weekend From Hell, or I could have written about ACTCIACTC's third blogbirthday. Maybe tomorrow. Meanwhile check out Grand Rounds Vol. II No.41 at Dr. Rangel's. |
Too bad I had the On Call Weekend From Hell, or I could have written about ACTCIACTC's third blogbirthday. Maybe tomorrow. Meanwhile check out Grand Rounds Vol. II No.41 at Dr. Rangel's. |
![]()





