Thursday, June 16, 2005
Share the Wealth...
Or pass the buck. From The Journal of Trauma:Workload Redistribution: A New Approach to the 80-Hour Workweek.

And hours:

There were no statisically significant difference in the number of missed injuries between the pre and post sample periods.
This paper was presented at the AAST meeting and inspired a lively discussion about the role of the trauma service and the specialist surgeon:
In reply(emphasis mine)....
So will we have a "captain-less" ship? |
Or pass the buck. From The Journal of Trauma:Workload Redistribution: A New Approach to the 80-Hour Workweek.
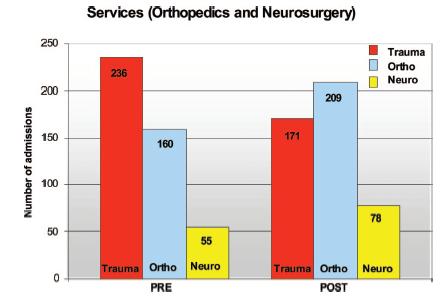
Background: The new Accreditation Council for Graduate Medical Education-mandated 80-hour resident work week has resulted in busy trauma services struggling to meet these strict guidelines, or face loss of accreditation.They analyzed the volume of trauma admissions between July and December 2002 (pre) and July to December 2003 (post). After July 2003 isolated neuro and orthopedic injuries would be admitted to the respective service. The six month totals were 543 and 549 patients. (my level II trauma center cares for almost as many patients). It seems they did reduce volume and improve workhour compliance, but altering the dynamic of the trauma service:
Methods: Beginning in July 2003, our Level I trauma service began a policy of direct admission of isolated neurosurgical or orthopedic injuries to the specific subspecialty service after complete evaluation by the trauma service in the emergency department for associated injuries. Complications, missed injuries, delayed diagnoses, and admission rates were compared in two 6-month periods: PRE, before the policy change; and POST, after the new policy had been instituted. Resident work hours were likewise compared over the two time periods.
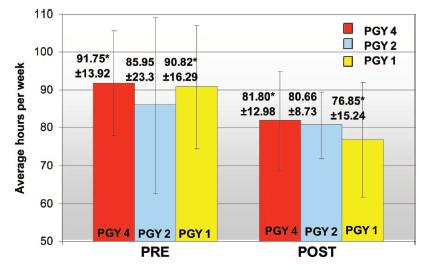
Results: Selected single-system injury admission to subspecialty services resulted in a 15% reduction in admissions to the trauma service. There were no significant differences in the overall complication rate, delayed diagnoses, or missed diagnoses between the PRE and POST time periods. Overall, there was a 9.7% reduction in resident work hours (p = 0.45; analysis of variance) between the PRE and POST periods, which allowed them, on average, to meet the Accreditation Council for Graduate Medical Education 80-hour workweek mandate.
Conclusion: Direct admission of patients with isolated injuries to subspecialty services is safe and decreases the workload of residents on busy trauma services.
It has been tradition that the trauma surgeon is captain of the ship, responsible for the oversight and care of the trauma patient. As a consequence of this tradition, all trauma patients are admitted for observation to the trauma services for at least 24 to 48 hours. During this period, subspecialty involvement is limited to a consultative role. The purpose of the period of observation is to avoid missed injuries and to expedite workup and diagnosis.The patients are initially evaluated by the trauma team and "farmed out" if the criteria are met. The results for admissions:
In 2003, the Accreditation Council for Graduate Medical Education (ACGME) mandated that residents in surgical specialties work no more than 80 hours per week. This ACGME mandate was enforced in July 2004. Because the trauma service is often the busiest surgical service in a hospital, innovative approaches to meet the 80-hour workweek mandate have been tried, including night float services, limited teaching services, and the involvement of midlevel providers in the care of the trauma patient.
The trauma service at Fletcher Allen Health Care/University of Vermont has been an American College of Surgeons-verified Level I trauma service since 1993. To meet the ACGME 80-hour workweek mandate, we altered our trauma protocol. We allowed selected patients with single-system injuries to be admitted to subspecialty services without a period of observation on the trauma service. This direct admission to subspecialty services was predicated on a full trauma evaluation by the trauma team in the emergency department at the time of admission. Our system incorporated a definition of single-system injury in which the main injury requiring subspecialty service admission had an Abbreviated Injury Scale (AIS)1 score of 3 or greater, with no other injuries of AIS score than 2. We hypothesized that this policy would reduce trauma resident workload and, in addition, would not increase delayed diagnoses or missed diagnoses.
And hours:
There were no statisically significant difference in the number of missed injuries between the pre and post sample periods.
This paper was presented at the AAST meeting and inspired a lively discussion about the role of the trauma service and the specialist surgeon:
Dr. Fred A. Luchette .....You have called this change in admitting service workload redistribution. Is it really a redistribution or just a shift of the workload to residents on the orthopedic and neurosurgery services? How has this impacted on their ability to comply with the 80-hour workweek? What effect has this practice had on the relationship between the residents on the various services? Do the orthopedic and neurosurgery residents feel the trauma service is dumping on them? What other changes were made by the general surgery residency program director so the residents would be compliant with the work hour restrictions? Convince me that the residents would not have been compliant with the 80-hour policy without this change by the trauma serviceConcerns over complication and the "presence" of the trauma service:
Dr. Sheldon Brotman.... You know one of the requirements in the gold book is that there should be a visible trauma service. The problem I have is when these patients go into orthopedics or neurosurgery, frequently the trauma residents become absolutely invisible. Although patients may go to subspecialty services the next day or two, I think trauma teams need to make rounds. They need to go back over the patient and look for missed injuries. In my own experience, it's frequently difficult to enforce that.......
Somehow, the complications that occur in orthopedics and neurosurgery aren't collected quite as carefully. Also, I don't think that the discharge process is really quite as facile in the other services either.
In reply(emphasis mine)....
Are we shifting the work to orthopedics and neurosurgery? Yes, but let's look at this. At our institution, over 90% of the operations performed on trauma patients are performed by subspecialty services.
If they are going to be performing the operations, isn't it appropriate that they take care of the patients afterward? The subspecialties can't have it both ways.
If they want to perform the operations, then they should take care of the patients in the perioperative period. Alternatively, if they are going to remain on our service, then maybe we should be performing some of these procedures, such as Dr. Cryer suggested in his presidential address.
I don't need to remind anyone in this room what a powerful negative disincentive it is for a medical student or resident, contemplating a career in trauma surgery, to see the trauma surgeons taking care of orthopedic or neurosurgical patients on their service after the subspecialty services have performed a huge operation with a huge professional component attached to it. To me, this borders almost on itinerant surgery.
So will we have a "captain-less" ship? |
![]()





