Saturday, June 18, 2005
Scan'em All and let God Sort Them Out II.....
A trio of articles again from this month's Journal of Trauma. The first:Spiral Computed Tomography for the Diagnosis of Cervical, Thoracic, and Lumbar Spine Fractures: Its Time has Come.
The sensitivity for plan radiographs from the study population are: 67% (6/9) for cervical fractures, 64% (7/11) for thoracic fractures, and 69% (11/16) for lumbar fractures. The next:Helical Computed Tomographic Scanning for the Evaluation of the Cervical Spine in the Unconscious, Intubated Trauma Patient.
The results of plain radiography:

Compared to helical CT:

And lastly, a meta-analysis:Computed Tomography Versus Plain Radiography to Screen for Cervical Spine Injury: A Meta-Analysis.
There have been other studies analyzing the accuracy of using the imaged vertebrae during chest and abdominal CT as a screening tool. Others have described the use of the initial "scout" views for that purpose as well. As the technology has advanced the concept of the "pan-scan": a CT of the head, total spine, chest, abdomen and pelvis has gained wider acceptance. Products such as the Statscan promise to bring such technology from the CT room to the resuscitation bay, as it has at the University of Maryland Shock-Trauma Center.
My own practice is to obtain CT scans of the cervical spine if the initial series is inadequate or is suspicious. I have not yet utilized spinal CT as a routine tool to evaluate the symptomatic or unconscious/intoxicated patient, but given these studies, I may begin to do so. |
A trio of articles again from this month's Journal of Trauma. The first:Spiral Computed Tomography for the Diagnosis of Cervical, Thoracic, and Lumbar Spine Fractures: Its Time has Come.
Background: Although the traditional method of diagnosing spine fractures (SF) has been plain radiography, Spiral Computed Tomography (SCT) is being used with increasing frequency. Our institution adopted SCT as the primary modality for the diagnosis of SF. The purpose of this study was to determine whether SCT scan can be used as a stand-alone diagnostic modality in the evaluation of SF.
Methods: Retrospective review of all blunt trauma patients over a two year period (1/01 - 12/02). Patients with neck pain, back pain, or spine tenderness underwent SCT of the symptomatic region. Patients who were unconscious or intoxicated underwent screening SCT of the entire spine. SCT was performed using 5 mm axial cuts with three-dimensional reconstructions in sagittal and coronal planes. Patients with a discharge diagnosis of cervical, thoracic, or lumbar SF were identified from the trauma registry by ICD-9 codes.
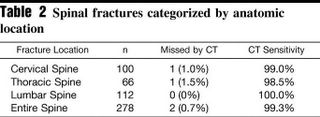
Results: There were 3,537 blunt trauma patients evaluated, with 236 (7%) sustaining a cervical, thoracic, or lumbar SF. Forty-five patients (19%) sustained a SF in more than one anatomic region. SCT missed SF in two patients. The cervical SF missed by SCT was a compression fracture identified by magnetic resonance imaging and was treated with a rigid collar. The thoracic SF missed by SCT was also a compression fracture identified on plain radiographs and required no treatment.
Conclusions: SCT of the spine identified 99.3% of all fractures of the cervical, thoracic, and lumbar spine, and those missed by SCT required minimal or no treatment. SCT is a sensitive diagnostic test for the identification of SF. Routine plain radiographs of the spine are not necessary in the evaluation of blunt trauma patients.

The sensitivity for plan radiographs from the study population are: 67% (6/9) for cervical fractures, 64% (7/11) for thoracic fractures, and 69% (11/16) for lumbar fractures. The next:Helical Computed Tomographic Scanning for the Evaluation of the Cervical Spine in the Unconscious, Intubated Trauma Patient.
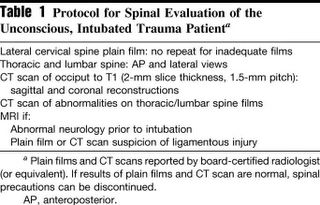
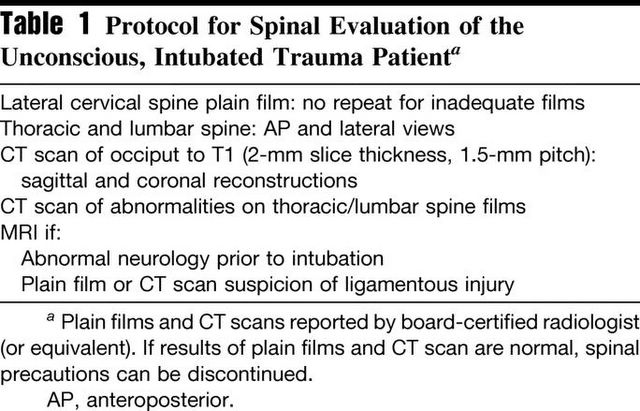
Background: Assessment of the spine in the unconscious trauma patient is limited by an inadequate clinical examination. The potential of a missed unstable disc or ligamentous injury results in many patients remaining immobilized in critical care units for prolonged periods.The protocol does not appear as strict as the first study:
Methods: This study evaluates helical computed tomographic (CT) scanning of the whole cervical spine as part of a spinal assessment and clearance protocol.
Results: Four hundred thirty-seven unconscious, intubated, blunt trauma patients underwent CT scanning of the cervical spine. Sixty-one patients had a cervical spine injury and 31 (7.0%) were unstable. CT scanning had a sensitivity of 98.1%, a specificity of 98.8%, and a negative predictive value of 99.7%. There were no missed unstable injuries. In contrast, an adequate lateral cervical spine film detected only 24 injuries (14 unstable), with a sensitivity of 53.3%.
Conclusion: Helical CT scanning of the cervical spine allows rapid and safe evaluation of the cervical spine in the unconscious, intubated trauma patient.
The results of plain radiography:

Compared to helical CT:

And lastly, a meta-analysis:Computed Tomography Versus Plain Radiography to Screen for Cervical Spine Injury: A Meta-Analysis.
Background: To compare the test performance of plain radiography and computed tomography (CT) in the detection of patients with cervical spine injuries following blunt traumatic events among those patients determined to require screening radiography.
Methods: We conducted a MEDLINE search for articles published from January 1995 through June 2004, manually reviewed bibliographies, and hand searched four journals. Studies were included if they contained data on the performance of both plain radiography and CT in the detection of patients with blunt cervical spine injuries. Both authors screened titles and abstracts identified by the search and seven of the 712 articles met all inclusion criteria. Both authors independently abstracted data from these seven studies and disagreements were resolved by mutual agreement.
Results: Patient entry criteria were highly variable for each study and there were no randomized controlled trials. For identifying patients with cervical spine injury, the pooled sensitivity for cervical spine plain radiography was 52% (95% CI 47, 56%) and for CT was 98% (95% CI 96, 99%). The test for heterogeneity suggests that significant differences exist between studies in the measurement of the sensitivity for plain radiography (p = 0.07). Due to limitations of the gold standard tests in each study, a calculation of a combined specificity was not possible.
Conclusion: Despite the absence of a randomized controlled trial, ample evidence exists that CT significantly outperforms plain radiography as a screening test for patients at very high risk of cervical spine injury and thus CT should be the initial screening test in those patients with a significantly depressed mental status. There is insufficient evidence to suggest that cervical spine CT should replace plain radiography as the initial screening test for less injured patients who are at low risk for cervical spine injury but still require a screening radiographic examination.
There have been other studies analyzing the accuracy of using the imaged vertebrae during chest and abdominal CT as a screening tool. Others have described the use of the initial "scout" views for that purpose as well. As the technology has advanced the concept of the "pan-scan": a CT of the head, total spine, chest, abdomen and pelvis has gained wider acceptance. Products such as the Statscan promise to bring such technology from the CT room to the resuscitation bay, as it has at the University of Maryland Shock-Trauma Center.
My own practice is to obtain CT scans of the cervical spine if the initial series is inadequate or is suspicious. I have not yet utilized spinal CT as a routine tool to evaluate the symptomatic or unconscious/intoxicated patient, but given these studies, I may begin to do so. |
![]()





