Tuesday, March 29, 2005
TV Review of Grey's Anatomy.....
When I first saw the ads for ABC's Grey's Anatomy I was intrigued. Life of a surgical resident in a primetime drama? That was something I could relate to. But would America watch residents rounding at six, to the OR at seven-thirty, clinic at two, and hopefully home at eight. Would they watch as the residents admitted appendicitis from the ED, held hook on an exploration in the OR, and slept, ate, or watched SportsCenter? Probably not.
Unfortunately the show does the usual job of distorting reality. How so? Let us count the ways:
Disregard for work hour limits: On duty for forty-eight hours straight? Please, give me a break. Is the 80-hour limit not exciting enough for prime time? Obviously not.
Specialty Mismatch I:What are surgical interns doing taking care of a seizure patient? Yes the patient eventually needed an operation, but wouldn't their time be better spent elsewhere?
Specialty Mismatch II:Rare indeed is the surgeon who one day is performing an appendectomy and the next day and the next day a coronary bypass. ER is equally guilty. Their alleged general surgeons did everything from liver resections to lumbar laminectomies.
Yes, yes, I know it is a television show and not even a member of the reality genre. But it's no wonder the lay public has such a misperception of how medicine really works when the airwaves are filled with such tripe. |
When I first saw the ads for ABC's Grey's Anatomy I was intrigued. Life of a surgical resident in a primetime drama? That was something I could relate to. But would America watch residents rounding at six, to the OR at seven-thirty, clinic at two, and hopefully home at eight. Would they watch as the residents admitted appendicitis from the ED, held hook on an exploration in the OR, and slept, ate, or watched SportsCenter? Probably not.
Unfortunately the show does the usual job of distorting reality. How so? Let us count the ways:
Disregard for work hour limits: On duty for forty-eight hours straight? Please, give me a break. Is the 80-hour limit not exciting enough for prime time? Obviously not.
Specialty Mismatch I:What are surgical interns doing taking care of a seizure patient? Yes the patient eventually needed an operation, but wouldn't their time be better spent elsewhere?
Specialty Mismatch II:Rare indeed is the surgeon who one day is performing an appendectomy and the next day and the next day a coronary bypass. ER is equally guilty. Their alleged general surgeons did everything from liver resections to lumbar laminectomies.
Yes, yes, I know it is a television show and not even a member of the reality genre. But it's no wonder the lay public has such a misperception of how medicine really works when the airwaves are filled with such tripe. |
Sunday, March 20, 2005
What Happens in Vegas...

I'll be away for a few days trying to learn a thing or two while gambling with the kid's college fund.
See you later this week. |
I'll be away for a few days trying to learn a thing or two while gambling with the kid's college fund.
See you later this week. |
Friday, March 18, 2005
Tales from the Trauma Service VII...
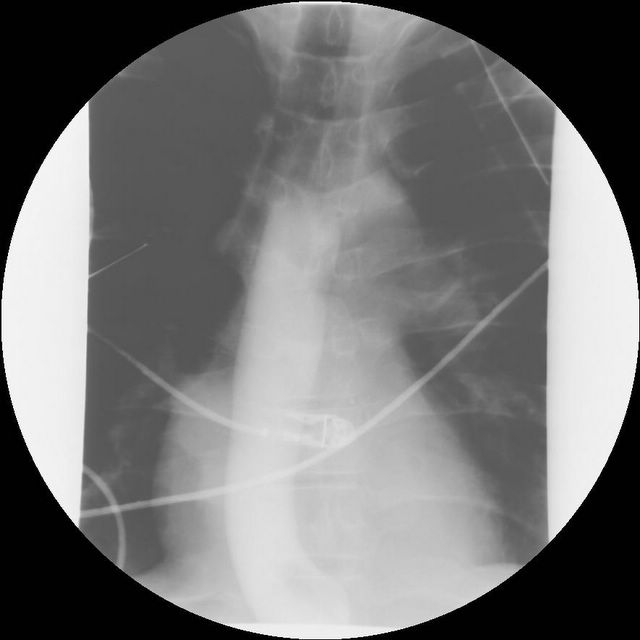
Sometimes millimeters make the difference. 20-ish year old shot in the right side of his back. He was tachycardic at the referring facility, but otherwise stable. No chest tubes were placed. Here is his initial CXR:
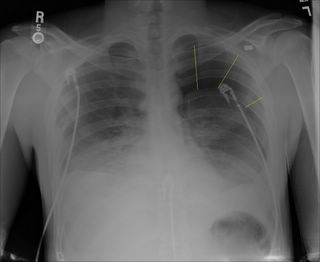
Interestingly the left pneumothorax and the bullet in the left side of his chest was not mentioned during the presentation. A better view (with some chest tubes) can be seen in the scout film of his CT:
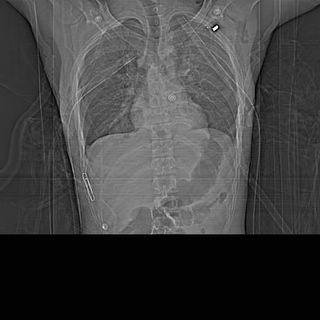
A paperclip marks the entry wound. Lots of vital things live between point "A" and point "B". Since he was hemodynamically stable he could undergo a complete radiographic evaluation instead of an exploration. After discussion with the radiologist he underwent a CT angiogram of his chest rather than a conventional angiogram:
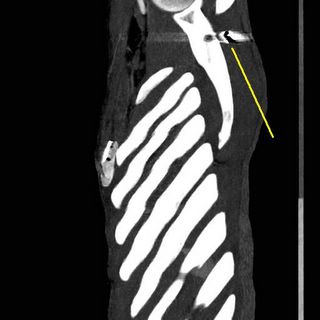
This is one of the leftmost slices of the reconstruction showing the projectile posterior to the left scapula.

The black line points to fragments anterior to the verterbral body. That is the bullet went in between the aorta and the verterbra. And this patient was real skinny, not a great deal of fat back there. Here is the AP view:
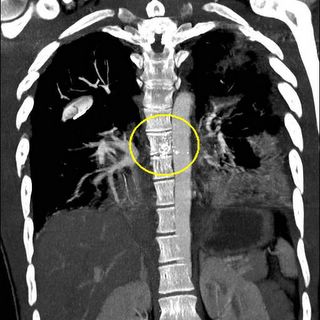
Really close there. So his aorta was OK. No air leak in his chest tubes and the path was too posterior to affect the airway. Next thing was the esophagus:

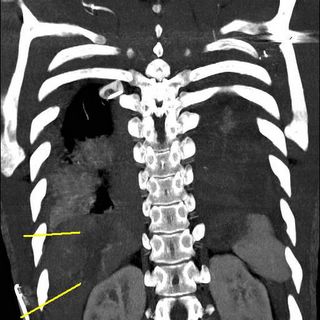
O.K. by barium swallow. But the CT of his abdomen also showed:


A injury to his liver. So the bullet had to penetrate the diaphragm at least once. Here are some images from the reconstruction:

Showing the tract of the projectile. The patient was still tachycardic but responding to fluids. Off to the OR.
The injury was difficult to expose due to its' location. The diaphragm injury was within the boundaries of the right triangular ligament through the "bare area" of the liver. The difficulty of exposure is one reason the treatment of retrohepatic venous injuries is so difficult. It was small, about the size of a .22 caliber projectile. A portal branch was ligated with a clip and the diffuse oozing was controlled with fibrin glue. Commercial hemostatic agents are available but the largest volume is 5cc. I make my own with cryoprecipitate, thrombin, and calcium. I can usually get 180 cc at least of glue. He required 2 units of blood. Anesthesia did a good job of keeping him warm and he actually went from 96.4 degrees to 98 degrees.
Transmediastinal wounds are difficult to take care of because of the multimodality apprach required. Patients that are hemodynamically unstable must be taken promptly to the OR. The rest must have their vascular and aerodigestive structures evaluated.
The gold standard used to be arch aortogram, bronchoscopy, and barium swallow. The advent of multi-slice CT scanning has largely reduced the use of the first two modalities, being reserved for inconclusive studies. Barium swallow still has its' role.
Just a few millimeters between life and death.....
Sometimes millimeters make the difference. 20-ish year old shot in the right side of his back. He was tachycardic at the referring facility, but otherwise stable. No chest tubes were placed. Here is his initial CXR:
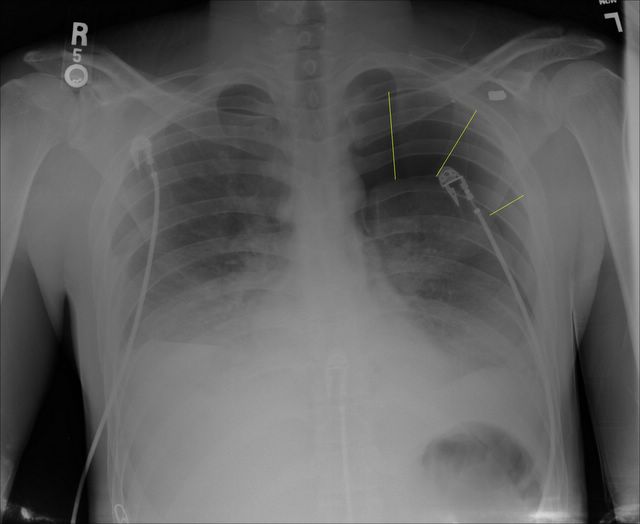
Interestingly the left pneumothorax and the bullet in the left side of his chest was not mentioned during the presentation. A better view (with some chest tubes) can be seen in the scout film of his CT:
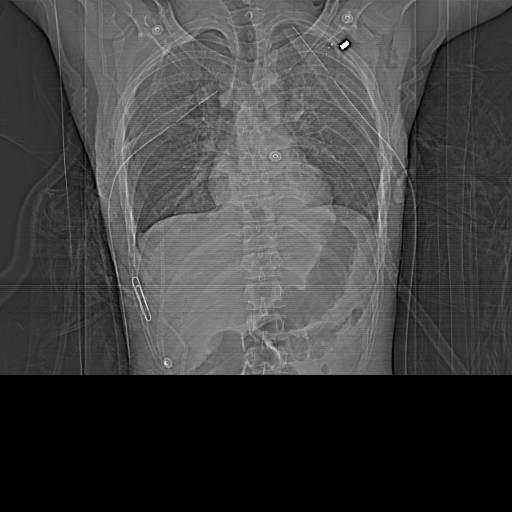
A paperclip marks the entry wound. Lots of vital things live between point "A" and point "B". Since he was hemodynamically stable he could undergo a complete radiographic evaluation instead of an exploration. After discussion with the radiologist he underwent a CT angiogram of his chest rather than a conventional angiogram:
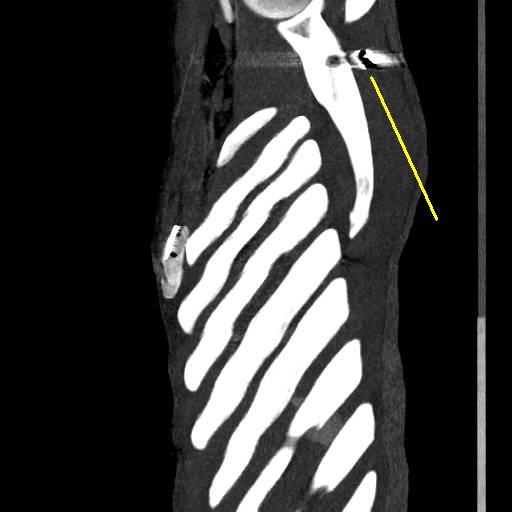
This is one of the leftmost slices of the reconstruction showing the projectile posterior to the left scapula.

The black line points to fragments anterior to the verterbral body. That is the bullet went in between the aorta and the verterbra. And this patient was real skinny, not a great deal of fat back there. Here is the AP view:

Really close there. So his aorta was OK. No air leak in his chest tubes and the path was too posterior to affect the airway. Next thing was the esophagus:
O.K. by barium swallow. But the CT of his abdomen also showed:


A injury to his liver. So the bullet had to penetrate the diaphragm at least once. Here are some images from the reconstruction:


Showing the tract of the projectile. The patient was still tachycardic but responding to fluids. Off to the OR.
The injury was difficult to expose due to its' location. The diaphragm injury was within the boundaries of the right triangular ligament through the "bare area" of the liver. The difficulty of exposure is one reason the treatment of retrohepatic venous injuries is so difficult. It was small, about the size of a .22 caliber projectile. A portal branch was ligated with a clip and the diffuse oozing was controlled with fibrin glue. Commercial hemostatic agents are available but the largest volume is 5cc. I make my own with cryoprecipitate, thrombin, and calcium. I can usually get 180 cc at least of glue. He required 2 units of blood. Anesthesia did a good job of keeping him warm and he actually went from 96.4 degrees to 98 degrees.
Transmediastinal wounds are difficult to take care of because of the multimodality apprach required. Patients that are hemodynamically unstable must be taken promptly to the OR. The rest must have their vascular and aerodigestive structures evaluated.
The gold standard used to be arch aortogram, bronchoscopy, and barium swallow. The advent of multi-slice CT scanning has largely reduced the use of the first two modalities, being reserved for inconclusive studies. Barium swallow still has its' role.
Just a few millimeters between life and death.....
Labels: Tales from the Trauma Service
|Tuesday, March 15, 2005
Valve Job...
From the New York Times: A Promising Recovery After a New Aortic Valve Procedure
From the New York Times: A Promising Recovery After a New Aortic Valve Procedure
A team of cardiologists in Michigan has implanted an artificial heart valve in a 76-year-old man by feeding the device through a vein in his left leg instead of opening his chest and stopping his heart.Alas, endovascular valve replacement is not for everyone:
The patient, Fernando Giangrande, had the three-hour procedure on Thursday, left the hospital on Sunday and was back at work yesterday customizing vintage cars at his Ford dealership. Replacement of the valve through open-heart surgery normally requires a week in the hospital and a longer total recovery time, assuming the patient was deemed strong enough to have the surgery in the first place.
The experimental implant was the first of at least 150 that federal regulators will require before considering approval of the technique for widespread use. But medical experts say the procedure could eventually extend the lives of many people who are too frail or ill to endure open-heart surgery. Failing valves are diagnosed in tens of thousands of Americans each year, and that number is expected to grow as baby boomers pass the age of 70.
Medical experts warn that even if the technique is mastered, the heart repairs may not last as long as those achieved through conventional surgery.I remember when stent-grafting for abdominal aneurysms was limited to the same set of patients. The procedure was not without difficulty:
Mr. Giangrande's doctor, Dr. William W. O'Neill, the chief of cardiology at Beaumont, said that in its current form, the technique is a last resort. "People who are good candidates for open-heart surgery should not even look into this," he said in a brief interview immediately after the procedure.
The first effort to deploy the valve failed when it became jammed in a passageway the team made through a wall in Mr. Giangrande's heart. When Dr. O'Neill tried to pull it back, the balloon inside the valve inflated. Unable to go forward, the team spent 30 minutes scrambling to move the valve back down the large vein that runs up the spine. They pinned it into the wall of the vessel just above his kidneys, where it is expected to have no impact on blood flow. A second artificial valve was attached to the catheter and, ultimately, successfully installedI guess they had to install the valve antegrade because they may have not been able to seat the valve against the flow. I wonder if they used adenosine to temporarily stop the heart during deployment? An exiting development to say the least. |
Grand Rounds XXV
Dr. Orac has the block time in the OR today, but spends most of it in the lounge watching TV waiting for his room to turn over. |
Dr. Orac has the block time in the OR today, but spends most of it in the lounge watching TV waiting for his room to turn over. |
Monday, March 14, 2005
From the Unusual Mechanism Injury Department.....
One of the reasons I like reading The Journal of Trauma is the large number of case reports that are published. Occasionally one will catch my eye, as one last month did:Pneumoperitoneum from Orogenital Insufflation: An Incidental Finding Resulting in Nontherapeutic Celiotomy:
A discussion of the cause and literature review follow.
So where in the secondary survey do I ask about this? |
One of the reasons I like reading The Journal of Trauma is the large number of case reports that are published. Occasionally one will catch my eye, as one last month did:Pneumoperitoneum from Orogenital Insufflation: An Incidental Finding Resulting in Nontherapeutic Celiotomy:
A restrained, 16-year-old female driver presented to our facility after her motor vehicle struck a tree. The patient admitted to falling asleep at the wheel and sustained a transient loss of consciousness. Primary survey found her to be hemodynamically stable, with a Glasgow Coma Scale score of 15. Secondary survey revealed seal belt distribution ecchymosis across her lower abdomen and chest, with mild abdominal pain and tenderness. She underwent an abdominal computed tomographic (CT) scan that showed a small amount of free air located within the lesser sac near the duodenum (Fig. 1). No extravasation of contrast, solid organ injury, or intrathoracic air was noted. She underwent exploration with the presumptive diagnosis of hollow viscus injury. On opening the abdomen, the hepatoduodenal ligament was free of fat and transparent, revealing several small bubbles of air just inside the opening to the lesser sac. This corresponded to the air seen on the CT scan. The air bubbles could be touched by inserting a finger into the foramen of Winslow. An extensive search revealed no intra-abdominal organ injury, bile staining, or remarkable free fluid. The stomach was occluded proximally and the duodenum was insufflated with air (under a pool of saline), with no evidence of leak. A careful sexual history was obtained postoperatively and revealed that the patient had forceful vaginal insufflation during oral sex in the previous 12 hours. No other source of reasonable explanation for the free air could be found. Her postoperative day course was unremarkable and she was discharged home on postoperative day 4.
A discussion of the cause and literature review follow.
So where in the secondary survey do I ask about this? |
Tales from the Trauma Service VI......
Day job and computer games taking their toll as of late. The gunshot wound to the buttocks is a frequent "comic relief" tool used in war movies such as Forrest Gump or Band of Brothers. But for a forty-ish year old over the weekend it was no laughing matter. He was shot with an entry wound very lateral in his left buttock. The projectile was located subcutaneously at his lateral right thigh. His urine was clear and gross blood on his rectal exam. His films:

The yellow circles mark the entry wound (with paper clip) and some soft tissue air near his scrotum.

And now we see the culprit. A digital rectal exam revealed a wound in his lower rectum or anus. He was too tender to allow for a proctoscopy in the ED. So off to the OR.
Sorry, not enough light for pictures. I will use my Netter atlas:
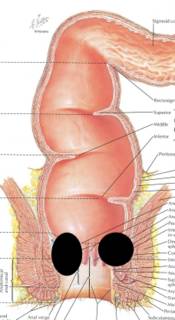
The black circles represent the areas of tissue damage to his posterior anus.
Here is another view:
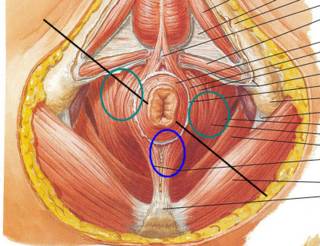
The black line is the approximate path of the projectile, the green circles are the areas of severely damaged external sphincter muscle, and the blue circle is the area of posterior attachment.
I tried to piece together things as best as I could. I also placed an end sigmoid colostomy. The usual plan is barium evaluation and anorectal manometry in a few months. The two main worries are incontinence and stricture. This may be a permanent colostomy for him.
He doesn't think its too funny.
Day job and computer games taking their toll as of late. The gunshot wound to the buttocks is a frequent "comic relief" tool used in war movies such as Forrest Gump or Band of Brothers. But for a forty-ish year old over the weekend it was no laughing matter. He was shot with an entry wound very lateral in his left buttock. The projectile was located subcutaneously at his lateral right thigh. His urine was clear and gross blood on his rectal exam. His films:
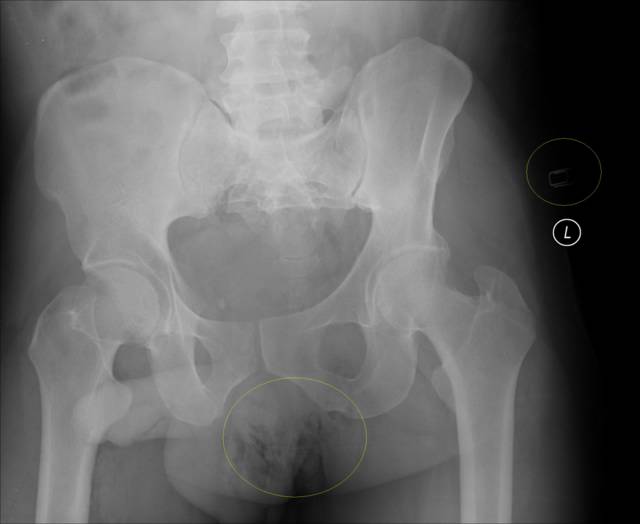
The yellow circles mark the entry wound (with paper clip) and some soft tissue air near his scrotum.

And now we see the culprit. A digital rectal exam revealed a wound in his lower rectum or anus. He was too tender to allow for a proctoscopy in the ED. So off to the OR.
Sorry, not enough light for pictures. I will use my Netter atlas:
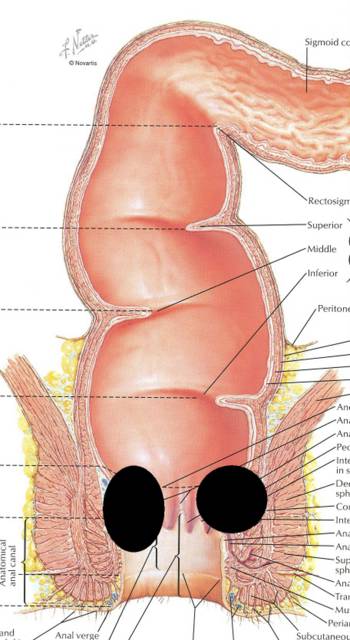
The black circles represent the areas of tissue damage to his posterior anus.
Here is another view:
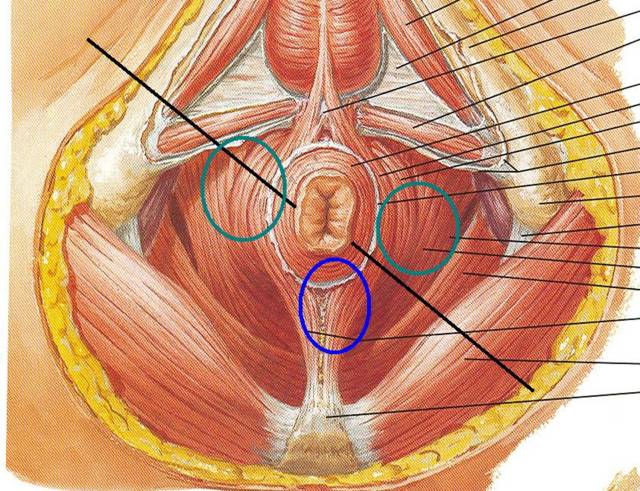
The black line is the approximate path of the projectile, the green circles are the areas of severely damaged external sphincter muscle, and the blue circle is the area of posterior attachment.
I tried to piece together things as best as I could. I also placed an end sigmoid colostomy. The usual plan is barium evaluation and anorectal manometry in a few months. The two main worries are incontinence and stricture. This may be a permanent colostomy for him.
He doesn't think its too funny.
Labels: Tales from the Trauma Service
|Tuesday, March 08, 2005
Saturday, March 05, 2005
Wednesday, March 02, 2005
The Use of Market Forces by the State.....
Medicaid in Georgia is a real mess. Reimbursement is lousy and many physicians do not participate. It is becoming an access issue in many parts of the state. So a bill has been introduced in the General Assembly to attempt to remedy the situation. From House Bill 73:
So if you don't participate in Medicaid, you are excluded from State Merit. Is this the right thing for the state to do? The state is not doing anything that many private insurance companies don't already do. That is, not allowing a physician to participate in the PPO (or premiere plan) without participating in the HMO (or basic plan). So is it any more "evil", for lack of a better word, for the state to do it?
Now if the law mandated participation in Medicaid as a condition of licensure, I would agree wholeheartedly that the state had gone too far. A state-mandated assessment of licensed physicians to start up a liability insurance company is out-of-bounds as well. What's the difference? Because the state is using it's oft debated monopoly on licensure to compel behavior beyond what is required for patient safety. But here the state is using the market (access to insured lives) to affect behavior. No physician has a "right" to participate in State Merit or Medicaid, anymore than they have the "right" to be on the provider panel for any commercial insurance plan.
I do this sort of thing all the time, but sort of backwards. If you don't consult me on insured patients during daylight hours, don't expect me to take care of your indigent cases in the middle of the night.
The specialists I have spoken to don't like it, since most of them have cut Medicaid patients from their practice, and would be faced with the decision as to whether continue to participate in State Merit.
The primary care physicians I have spoken to love it. They hope that this will help to end some of the difficulties they have had in getting patients to see specialists.
The bill doesn't appear to me moving very fast, so things may not change. |
Medicaid in Georgia is a real mess. Reimbursement is lousy and many physicians do not participate. It is becoming an access issue in many parts of the state. So a bill has been introduced in the General Assembly to attempt to remedy the situation. From House Bill 73:
A physician, as defined in Code Section 43-34-20, who participates in the state employeeś health insurance plan as provided for by Article 1 of Chapter 18 of Title 45 or in the board of regentś health insurance plan as provided for by subsection (e) of Code Section 31-5A-4 shall be required to participate in the Medicaid program. If at any point a physician is no longer eligible or declines to participate in the Medicaid program, such physician shall no longer be eligible to participate in either the state employee's or the board of regent's health insurance plan
So if you don't participate in Medicaid, you are excluded from State Merit. Is this the right thing for the state to do? The state is not doing anything that many private insurance companies don't already do. That is, not allowing a physician to participate in the PPO (or premiere plan) without participating in the HMO (or basic plan). So is it any more "evil", for lack of a better word, for the state to do it?
Now if the law mandated participation in Medicaid as a condition of licensure, I would agree wholeheartedly that the state had gone too far. A state-mandated assessment of licensed physicians to start up a liability insurance company is out-of-bounds as well. What's the difference? Because the state is using it's oft debated monopoly on licensure to compel behavior beyond what is required for patient safety. But here the state is using the market (access to insured lives) to affect behavior. No physician has a "right" to participate in State Merit or Medicaid, anymore than they have the "right" to be on the provider panel for any commercial insurance plan.
I do this sort of thing all the time, but sort of backwards. If you don't consult me on insured patients during daylight hours, don't expect me to take care of your indigent cases in the middle of the night.
The specialists I have spoken to don't like it, since most of them have cut Medicaid patients from their practice, and would be faced with the decision as to whether continue to participate in State Merit.
The primary care physicians I have spoken to love it. They hope that this will help to end some of the difficulties they have had in getting patients to see specialists.
The bill doesn't appear to me moving very fast, so things may not change. |
Tuesday, March 01, 2005
I'm Coo-Coo for Co Co....
While EneMan has not made an appearance in River City we have been honored by the appearance of Co Co the Colossal Colon. Co Co had about 3500 visitors during its' stay, and the founders of The Colon Club Ms. McMasters and Ms. Volger gave a stirring and inspirational talk. Another of their projects is the Colondar a well-done wall calendar with 12 models, all diagnosed with colon cancer younger than age 50.
So go get your colonscopy!! |
While EneMan has not made an appearance in River City we have been honored by the appearance of Co Co the Colossal Colon. Co Co had about 3500 visitors during its' stay, and the founders of The Colon Club Ms. McMasters and Ms. Volger gave a stirring and inspirational talk. Another of their projects is the Colondar a well-done wall calendar with 12 models, all diagnosed with colon cancer younger than age 50.
So go get your colonscopy!! |
Curbside Pickup Available...
Or eat in and use the good china and silver.Grand Rounds XXIII served with a smile by Maria at intueri. |
Or eat in and use the good china and silver.Grand Rounds XXIII served with a smile by Maria at intueri. |
![]()





