Thursday, March 30, 2006
Tales From the Operating Room VIII.....
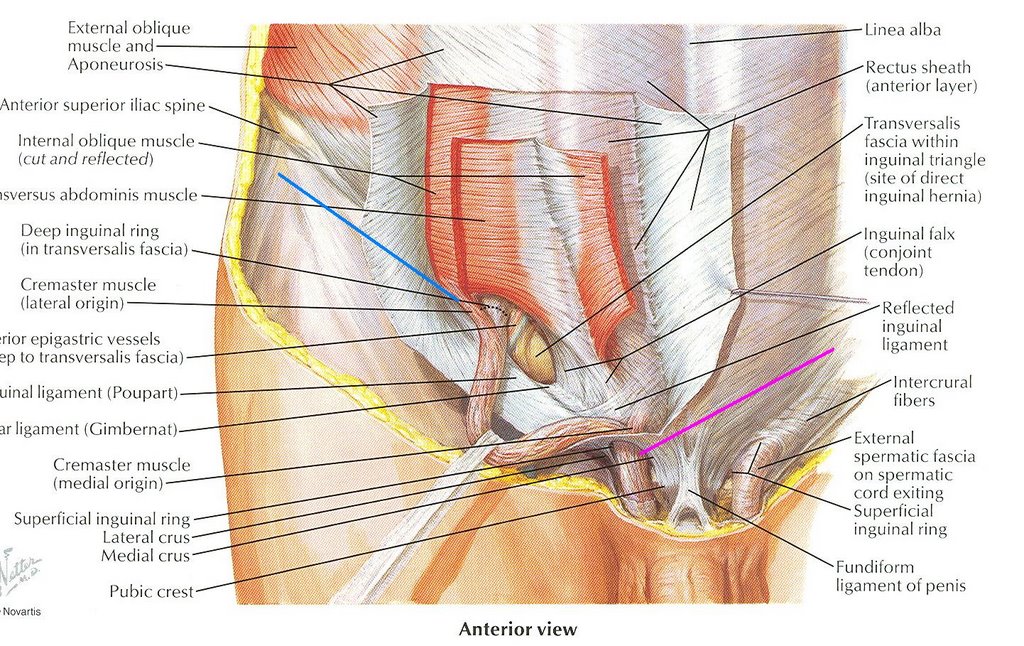
Paying back the man for last weeks misdeeds. Many transgressions were made up for by this case, left for me on call by my partner. 30-ish with incarcerated bilateral hernias. Started on the right side. The scrotum was quite large but he had little distance between his internal and external rings, which are demonstrated below:

This left little room to work in. I had to enter the sac to withdraw the hernia contents from the scrotum. Look what I reeled in:

Looks to be his entire greater omentum had found a home in his scrotum. With his scrotum "decompressed" I was able to ascertain he had no large hernia on the left. I dissected out the sac and isolated the important testicular stuff. I then placed the omentum back in the sac:

Unfortunately his scrotum didn't show up too well in these pictures. I did this to try to facilitate the placement of the omentum back into the abdomen. This, along with increased paralytics, steep trendelenberg position, and 45 minutes of effort could not get it back inside. I elected not to extend his internal ring because his tissue was pretty weak. I tried stuffing it back in independent of the sac, but created bleeding by doing so. I ended up resecting about 60 percent of it and repaired him in my usual plug-and-patch fashion.
Paying back the man for last weeks misdeeds. Many transgressions were made up for by this case, left for me on call by my partner. 30-ish with incarcerated bilateral hernias. Started on the right side. The scrotum was quite large but he had little distance between his internal and external rings, which are demonstrated below:
This left little room to work in. I had to enter the sac to withdraw the hernia contents from the scrotum. Look what I reeled in:

Looks to be his entire greater omentum had found a home in his scrotum. With his scrotum "decompressed" I was able to ascertain he had no large hernia on the left. I dissected out the sac and isolated the important testicular stuff. I then placed the omentum back in the sac:

Unfortunately his scrotum didn't show up too well in these pictures. I did this to try to facilitate the placement of the omentum back into the abdomen. This, along with increased paralytics, steep trendelenberg position, and 45 minutes of effort could not get it back inside. I elected not to extend his internal ring because his tissue was pretty weak. I tried stuffing it back in independent of the sac, but created bleeding by doing so. I ended up resecting about 60 percent of it and repaired him in my usual plug-and-patch fashion.
Labels: Tales from the Operating Room
|Monday, March 20, 2006
Friday, March 17, 2006
Match Stats 2006...
The annual exercise of medical student flagellation took place yesterday. The review of the statistics provide a glimpse of how medical students are voting with their feet.
General surgery offered 1047 positions this year, down from 1051 in 2005. US graduates filled 872 (83%) of these slots. This is down slightly from last year as well, with 885 positions filled by US graduates, but the percentage of slots filled by US graduates rose from 80%. Only one slot remained unfilled.
Family practice offered 2711 positions, fifty less than in 2005. 2307 (85%) were filled. This is increased from the 82% fill percentage from last year. 1123 were filled by US graduates (48.6%). This percentage is roughly the same as last year. Keep in mind that as recently as 2003, 2900 slots were available in family practice.
Internal medicine had 4735 slots available, down from 4768 last year. Of these 4636 were filled (97%), the same as last year. 2668 positions filled by US students (58%), up slightly.
Pediatrics filled 2209 of 2288 positions (97%). As in 2005 the total number of slots and percentage filled rose, unique among the primary care specialties. 1668 of these were filled by US graduates (75.5%), a slight percentage decline from last year.
If the number of positions offered were the same as last year, FP would have a 83.6% fill and IM would have the same 97%.
OB/GYN offered 1154 positions, up from 1144 last year. 1130 were filled (98%), up from the 97.4% last year. If the number of positions remained static, the fill percentage would have been 98.8 percent. 835 (73.9%) were filled by US grads.
Anesthesia had a fill percentage of 97.6%, up from 94.8 last year. This with an increase of 89 offered positions. More positions were filled this year than were offered last year.
Radiology offered 129 positions, down from 134 last year, but up from 126 from 2004. Fill percentage of 95.3% this year, up from 92.5%
EM filled 1218 of 1251 positions (97.4%). This is an increase of offered positions from 1188 with a slight fall in fill percentage (98%).
What does it mean? Primary care remains relatively static but their fill rates are not rising to meet the demand of an aging population. Has it reached the bottom? Surgery and OB/GYN are increasingly competitive. A consequence of workhour limits perhaps? Anesthesia is wildly popular.
Continue to track and trend as they say. |
The annual exercise of medical student flagellation took place yesterday. The review of the statistics provide a glimpse of how medical students are voting with their feet.
General surgery offered 1047 positions this year, down from 1051 in 2005. US graduates filled 872 (83%) of these slots. This is down slightly from last year as well, with 885 positions filled by US graduates, but the percentage of slots filled by US graduates rose from 80%. Only one slot remained unfilled.
Family practice offered 2711 positions, fifty less than in 2005. 2307 (85%) were filled. This is increased from the 82% fill percentage from last year. 1123 were filled by US graduates (48.6%). This percentage is roughly the same as last year. Keep in mind that as recently as 2003, 2900 slots were available in family practice.
Internal medicine had 4735 slots available, down from 4768 last year. Of these 4636 were filled (97%), the same as last year. 2668 positions filled by US students (58%), up slightly.
Pediatrics filled 2209 of 2288 positions (97%). As in 2005 the total number of slots and percentage filled rose, unique among the primary care specialties. 1668 of these were filled by US graduates (75.5%), a slight percentage decline from last year.
If the number of positions offered were the same as last year, FP would have a 83.6% fill and IM would have the same 97%.
OB/GYN offered 1154 positions, up from 1144 last year. 1130 were filled (98%), up from the 97.4% last year. If the number of positions remained static, the fill percentage would have been 98.8 percent. 835 (73.9%) were filled by US grads.
Anesthesia had a fill percentage of 97.6%, up from 94.8 last year. This with an increase of 89 offered positions. More positions were filled this year than were offered last year.
Radiology offered 129 positions, down from 134 last year, but up from 126 from 2004. Fill percentage of 95.3% this year, up from 92.5%
EM filled 1218 of 1251 positions (97.4%). This is an increase of offered positions from 1188 with a slight fall in fill percentage (98%).
What does it mean? Primary care remains relatively static but their fill rates are not rising to meet the demand of an aging population. Has it reached the bottom? Surgery and OB/GYN are increasingly competitive. A consequence of workhour limits perhaps? Anesthesia is wildly popular.
Continue to track and trend as they say. |
Wednesday, March 15, 2006
Hard Out Here for a Pimp.....
From the New York Times:Young Doctors Learn Quickly in the Hot Seat
Let's activate the Bard Parker Internet wayback machine to July of 2003 and a discussion of Pimping, Surgeon-Style
Ahh, the memories... |
From the New York Times:Young Doctors Learn Quickly in the Hot Seat
A favorite time to grill students has been on rounds, when doctors and students examine hospitalized patients. Here, senior attending physicians may ask students to list the various types of lymphomas, point out structures on X-rays, describe clotting disorders or choose among antibiotics.
At times, particular students are singled out, especially if they are following the patient in question. If the student is having difficulty and the senior doctor keeps pushing, rounds may suddenly become very uncomfortable. At other times, other students or resident physicians may be allowed to bail out their colleagues.
Let's activate the Bard Parker Internet wayback machine to July of 2003 and a discussion of Pimping, Surgeon-Style
Poking around the othe medblogs and came across this post about "pimping" at Force of Mouth. While written from an internists standpoint it strikes a chord with me and my experience in residency as pimping is described as how the "shame-based motivational system of medical education is applied". See, a surgical residency is at least five years of shame based motivation. Surgeons can be sadistic bastards with very little encouragement. I mean, how many students have been driven from medicine teaching rounds in tears because they cannot answer questions. Seen it twice on the vascular service where I trained. In addition to the categories described in the piece, there are some pimping situations unique to surgery:
HEY, WHAT'S THIS? The most basic pimping in the OR. The living anatomy lesson.
WHY ARE WE DOING THIS OPERATION? What other options are there? This and the anatomy quiz described above are student and intern-level pimps.
WHAT CAN YOU DO IF YOU....cut the ureter, divide the common bile duct, find cancer everywhere.,ect...? This is a midlevel/Chief Resident level pimp. Usually there are five solutions to each problem, and if you can only name four you receive a butt-chewing so bad you need a colostomy.
The above games are simply a warm-up for the weekly pimp-fest that is the SURGICAL MORBIDITY AND MORTALITY conference. This is where you get up in front of all of the attendings an residents an present your complications. Lots of blood in the water here. Best part is where the attending of the case presented : 1.Disavows you ("Well, thats not how it really happened......") or 2. Nearly comes to blows with another attending over how the case was handled. "Bluffs" as described in the post usually result in the hapless resident being led down a path that results in the death of the patient in a spectacular fashion.
All of this is supposed to prepare the budding surgeon for his AMERICAN BOARD OF SURGERY CERTIFYING EXAMINATION or THE ORALS. This is you and about thirty other poor souls in suits sitting in hotel rooms being slow-roasted by examiners. And you pay $800 for the pleasure. Bluffing is treated as above, but you also fail the exam and get to pay to take another beating in a year's time. According to the board the pass rate for last year was 83 percent.
Ahh, the memories... |
Tuesday, March 14, 2006
Tuesday, March 07, 2006
EMTALA and Grand Rounds.....
Nobody is turned away from the emergency room. Submit to your Medical Screening Examination during Grand Rounds Vol. II No. 24. |
Nobody is turned away from the emergency room. Submit to your Medical Screening Examination during Grand Rounds Vol. II No. 24. |
Monday, March 06, 2006
Too Damn Lazy.....
Dr. Parker spends a great deal of time on hospital committees. I attend six regular committee meetings a month at Big Hospital. The newest addition to my toils is the Critical Care Multidisciplinary Committee (CCMC). Big Hospital is trying to make some major improvements to the delivery of care to really sick people.
One of the first things on the agenda was about physician supervision of the housestaff. Big Hospital has a Family Practice residency program, and these residents cover many services. The Staff Medicine service (the main target of this proposed policy) is staffed 75 percent of the time by private attendings, the other 25 percent by the sole hospitalist. These attendings are either FP's, primary care IM's, or medical subspecialists. They rotate two weeks at a time and are compensated for their teaching. They also bill and collect through the hospital. The CCMC felt that such supervision was lacking, IMHO it was totally non-existent. Motions were made and seconded and amended. What came out was a policy that read in part:
Reasonable, no? Certainly a patient ill enough to require critical care is ill enough to require evaluation by their attending physician, the physician ultimately responsible for their care. Aren't they?
Before this went to the medical executive committee this went to the internal medicine committee for their input.
It was akin to somebody dropping their pants and leaving a steaming pile on the conference room table. Physicians came with resignation letters for the teaching staff. The hue and cry was such that the chief of internal medicine promised to try and get it changed.
The chief then brings his concerns to med exec. I was at this meeting as he relayed their concerns. He and I went back-and-forth. His fist point:
Second point:
1) If boarded in IM and your specialty (as some are) that argument is a Non sequitur.
2) This would imply that the knowledge base of a first or second year FP resident trumps your years of experience in giving a patient heparin, nitroglycerine, and aspirin. Yes, such decisions about catheterization and thrombolytics are best reserved for a cardiologist, but the input of an experienced attending can avoid errors of omission and judgment. So you can at least keep the resident from screwing up. (When this was brought up he was unable to agree to that with a straight face)
3) If you feel uncomfortable handling those patients, maybe you should not be on the call roster.
My final point was to bring up the old "properly supervised housestaff can do no wrong" quote.
I was later told that an additional point had been brought up that the physicians in question had no problem with such a policy for private patients, but would not agree to this for the staff patients. Hence the title of this post. These are the same physicians who piss and moan about how bad the residents are. Well based on their behavior I can't really hold the residents fully responsible since those that are supposed to be teaching them can't get into the hospital to see a critically ill patient within four hours. When those who are supervising them refuse to take their calls in the middle of the night, or are so loathsome when called they create a culture of fear in the residents. When a resident pleads for help and is told to "do what you can" and "I'm not coming in". What a wonderful example we are setting for them.
Such is the rant bottled up over a long weekend of call. I'm sure you have stories of lazy as hell surgeons as well. Post'em in the comments. I'm going to take a nap. |
Dr. Parker spends a great deal of time on hospital committees. I attend six regular committee meetings a month at Big Hospital. The newest addition to my toils is the Critical Care Multidisciplinary Committee (CCMC). Big Hospital is trying to make some major improvements to the delivery of care to really sick people.
One of the first things on the agenda was about physician supervision of the housestaff. Big Hospital has a Family Practice residency program, and these residents cover many services. The Staff Medicine service (the main target of this proposed policy) is staffed 75 percent of the time by private attendings, the other 25 percent by the sole hospitalist. These attendings are either FP's, primary care IM's, or medical subspecialists. They rotate two weeks at a time and are compensated for their teaching. They also bill and collect through the hospital. The CCMC felt that such supervision was lacking, IMHO it was totally non-existent. Motions were made and seconded and amended. What came out was a policy that read in part:
A patient requiring admission to the intensive care unit must be evaluated by the attending physician within four hours of admission.
Reasonable, no? Certainly a patient ill enough to require critical care is ill enough to require evaluation by their attending physician, the physician ultimately responsible for their care. Aren't they?
Before this went to the medical executive committee this went to the internal medicine committee for their input.
It was akin to somebody dropping their pants and leaving a steaming pile on the conference room table. Physicians came with resignation letters for the teaching staff. The hue and cry was such that the chief of internal medicine promised to try and get it changed.
The chief then brings his concerns to med exec. I was at this meeting as he relayed their concerns. He and I went back-and-forth. His fist point:
The patient was seen by an ED physician and the resident, and that should be enough.It is not the ED physicians responsibility to formulate a treatment plan for a patient, but to diagnose immediate threats and stabilize the patient. Taken to a logical conclusion this reasoning would allow the ED physician to become a "uber hospitalist", or eliminate the ED physician entirely and have the on call guys sitting around the ED an have the patients triaged to them.
Second point:
The medical specialists have little to add to patients whose conditions lie outside of their field. The example given was a gastroenterologist caring for a patient with chest pain.My rebuttal points:
1) If boarded in IM and your specialty (as some are) that argument is a Non sequitur.
2) This would imply that the knowledge base of a first or second year FP resident trumps your years of experience in giving a patient heparin, nitroglycerine, and aspirin. Yes, such decisions about catheterization and thrombolytics are best reserved for a cardiologist, but the input of an experienced attending can avoid errors of omission and judgment. So you can at least keep the resident from screwing up. (When this was brought up he was unable to agree to that with a straight face)
3) If you feel uncomfortable handling those patients, maybe you should not be on the call roster.
My final point was to bring up the old "properly supervised housestaff can do no wrong" quote.
I was later told that an additional point had been brought up that the physicians in question had no problem with such a policy for private patients, but would not agree to this for the staff patients. Hence the title of this post. These are the same physicians who piss and moan about how bad the residents are. Well based on their behavior I can't really hold the residents fully responsible since those that are supposed to be teaching them can't get into the hospital to see a critically ill patient within four hours. When those who are supervising them refuse to take their calls in the middle of the night, or are so loathsome when called they create a culture of fear in the residents. When a resident pleads for help and is told to "do what you can" and "I'm not coming in". What a wonderful example we are setting for them.
Such is the rant bottled up over a long weekend of call. I'm sure you have stories of lazy as hell surgeons as well. Post'em in the comments. I'm going to take a nap. |
Sunday, March 05, 2006
Saturday, March 04, 2006
Can't Drive 55.....
From the Atlanta Journal-Constitution:Drive 55, try to stay alive
Watch the video here. |
From the Atlanta Journal-Constitution:Drive 55, try to stay alive
They knew it was dangerous.Talk about road rage.
"We could have really been hurt," said one of the Atlanta college students after their experiment.
"I was pretty sure that I was doing something stupid," said another.
That may be true. But, young and brash, they had a plan.
They wanted to go the speed limit on I-285.
In four cars, on all four lanes, the students from Georgia State University and other local colleges paced the entire midmorning flow of Perimeter traffic behind them at 55 mph for half an hour. They call it "an act of civil obedience."
"I get a lot of tickets," said Andy Medlin, 20, the Georgia State student who came up with the idea. "The best way to expose the flaws in the system is by following it."
Thankfully, they survived unharmed, though much maligned. The eight students captured it all on video for a student film competition, and the five-minute piece has fired up the country this week on blogs, talk radio, and national news broadcasts.
There was little doubt what the students' companions on the road thought that sunny Friday in January. The video shows drivers' steadily mounting hostility to the blockade. Cars honk. They drive onto the shoulder to speed around the students. Obscene gestures are made. The money shot, however, was captured beautifully by Hunter, who stood with her camera on the Church Street bridge over I-285 to watch the approaching traffic.
What she saw was ... nothing. An empty highway, with one or two stray cars. And then, like the hordes on the horizon, over the rise come the students backed by a phalanx of cars, cars, cars. The film plays it for all it's worth, bouncing the image back and forth to the funky beat of the Guru Fish song "Plush."
Watch the video here. |
Friday, March 03, 2006
Trauma Center Confusion.....
Some comments from this post bring up a point I neglected to make:
Designation of trauma centers is handled by the state or some other governing body. The requirements they use vary but are probably close the ACS's "Resources for Optimal Care of the Injured Patient", or as it is more widely known "the Gold Book":
The State of Georgia uses the "Gold Book" as its' measuring stick for trauma centers. Grady, MCCG (Macon), MCG (Augusta), and Memorial (Savannah) are all state designated trauma centers in Georgia. Shock-Trauma at UM is designated by the State of Maryland as is Harborview by the State of Washington.
On the patient care side of the equation I have little doubt that these three centers could easily pass ACS muster. But since a good deal of the review has to do with "systems" issues, I cannot give a sweeping statement about if they could become verified.
Verification, OTOH, is a voluntary process that a trauma center may undergo at which time it is inspected by members of the Consultation/Verification committee chosen by the ACS. The review involves a site visit and a chart review. Such a review may be more intense than one put on by the state. Why are such noted trauma centers as those listed above not verified? Verification is an expensive process. A verification visit costs $9000, a fee that does not include hotel and travel expenses of the reviewers. A re-designation is $8000, plus expenses, and re-designation occurs every three years. Some states which generously support their trauma centers tie in that funding to verification. This is probably why Ohio has 31 trauma centers of various levels. So it has to be financially worthwhile to undergo the process.
What about the prestige of being an ACS verified trauma center? The big dogs are probably secure enough with their reputations that they may regard verification as superfluous. As far as patient flow, in many places the trauma patients are going to flow to the same hospital, whether it is a trauma center or not. So verification may not produce many benefits.
As trauma systems nationwide become more evolved the requirement of ACS verification may be tied into funding. This would most certainly result in higher levels of ACS verification. |
Some comments from this post bring up a point I neglected to make:
I notice there aren't any ACS certified trauma centers in Maryland, either. Does UMM's R Adams Cowley Shock Trauma Center not conform to ACS's standards?and
I'm a bit perplexed myself, this list is obviously devoid of some major trauma centers (Emory in Atlanta, Harborview in Seattle, Shock Trauma in Baltimore). All three of these states (GA,WA,MD) are listed as being without level one trauma centers, yet these three are all superb trauma hospitals. The ACS list therefore might not be the most useful for making these observations... That being said, very interesting data, although not too surprising.First off let me explain the difference between designation and verification.
Designation of trauma centers is handled by the state or some other governing body. The requirements they use vary but are probably close the ACS's "Resources for Optimal Care of the Injured Patient", or as it is more widely known "the Gold Book":
The State of Georgia uses the "Gold Book" as its' measuring stick for trauma centers. Grady, MCCG (Macon), MCG (Augusta), and Memorial (Savannah) are all state designated trauma centers in Georgia. Shock-Trauma at UM is designated by the State of Maryland as is Harborview by the State of Washington.
On the patient care side of the equation I have little doubt that these three centers could easily pass ACS muster. But since a good deal of the review has to do with "systems" issues, I cannot give a sweeping statement about if they could become verified.
Verification, OTOH, is a voluntary process that a trauma center may undergo at which time it is inspected by members of the Consultation/Verification committee chosen by the ACS. The review involves a site visit and a chart review. Such a review may be more intense than one put on by the state. Why are such noted trauma centers as those listed above not verified? Verification is an expensive process. A verification visit costs $9000, a fee that does not include hotel and travel expenses of the reviewers. A re-designation is $8000, plus expenses, and re-designation occurs every three years. Some states which generously support their trauma centers tie in that funding to verification. This is probably why Ohio has 31 trauma centers of various levels. So it has to be financially worthwhile to undergo the process.
What about the prestige of being an ACS verified trauma center? The big dogs are probably secure enough with their reputations that they may regard verification as superfluous. As far as patient flow, in many places the trauma patients are going to flow to the same hospital, whether it is a trauma center or not. So verification may not produce many benefits.
As trauma systems nationwide become more evolved the requirement of ACS verification may be tied into funding. This would most certainly result in higher levels of ACS verification. |
Wednesday, March 01, 2006
Practice Makes Perfect V ......
From the January 26th issue of the New England Journal of Medicine:A National Evaluation of the Effect of Trauma-Center Care on Mortality. The abstract:
So level 1 centers do better with particularly nasty injuries (severe liver trauma, aortic, vena cava, iliac vascular, and penetrating cardiac injuries). However level 1 centers are hard to come by. Viewing the listing here, one notices the absence of verified ACS trauma centers of ANY level in Alabama, Florida, Georgia, South Carolina, or Tennessee.
Currently in Georgia legislature is forming a study committee to work on establishing a statewide trauma network. Safe America has launched an awareness program that includes public service announcements
From the January 26th issue of the New England Journal of Medicine:A National Evaluation of the Effect of Trauma-Center Care on Mortality. The abstract:
Background Hospitals have difficulty justifying the expense of maintaining trauma centers without strong evidence of their effectiveness. To address this gap, we examined differences in mortality between level 1 trauma centers and hospitals without a trauma center (non-trauma centers).One caveat the authors put forth:
Methods Mortality outcomes were compared among patients treated in 18 hospitals with a level 1 trauma center and 51 hospitals non-trauma centers located in 14 states. Patients 18 to 84 years old with a moderate-to-severe injury were eligible. Complete data were obtained for 1104 patients who died in the hospital and 4087 patients who were discharged alive. We used propensity-score weighting to adjust for observable differences between patients treated at trauma centers and those treated at non-trauma centers.
Results After adjustment for differences in the case mix, the in-hospital mortality rate was significantly lower at trauma centers than at nonÂtrauma centers (7.6 percent vs. 9.5 percent; relative risk, 0.80; 95 percent confidence interval, 0.66 to 0.98), as was the one-year mortality rate (10.4 percent vs. 13.8 percent; relative risk, 0.75; 95 percent confidence interval, 0.60 to 0.95). The effects of treatment at a trauma center varied according to the severity of injury, with evidence to suggest that differences in mortality rates were primarily confined to patients with more severe injuries.
Conclusions Our findings show that the risk of death is significantly lower when care is provided in a trauma center than in a non-trauma center and argue for continued efforts at regionalization.
Caution is needed in generalizing our results. Because the NSCOT is a study of the effectiveness of trauma centers in urban and suburban America, our results cannot readily be extrapolated to rural areas of the country. In addition, we did not address the relative effectiveness of intermediate levels (2, 3, or 4) of trauma care.Ask and ye shall receive. From the Journal of the American College of Surgeons:Relationship Between American College of Surgeons Trauma Center Designation and Mortality in Patients with Severe Trauma (Injury Severity Score > 15):
BackgroundThe unadjusted mortality rates were better at level 1 centers versus level 2 centers (14.9 vs. 15.4 percent). But adjustments by logistic regression were required to achieve statistical significance.
We studied the association of the American College of Surgeons (ACS) trauma center designation and mortality in adult patients with severe trauma (Injury Severity Score > 15). ACS designation of trauma centers into different levels requires substantial financial and human resources commitments. There is very little work published on the association of ACS trauma center designation and outcomes in severe trauma.
Study design
National Trauma Data Bank study including all adult trauma admissions (older than 14 years of age) with Injury Severity Score (ISS) > 15. The relationship between ACS level of trauma designation and survival outcomes was evaluated after adjusting for age, mechanism of injury, ISS, hypotension on admission, severe liver trauma, aortic, vena cava, iliac vascular, and penetrating cardiac injuries.
Results
A total of 130,154 patients from 256 trauma centers met the inclusion criteria. Adjusted mortality in ACS-designated Level II centers and undesignated centers was notably higher than in Level I centers (adjusted odds ratio, 1.14; 95% CI, 1.09−120; p <> 15 treated in ACS Level I trauma centers have considerably better survival outcomes than those treated in ACS Level II centers
So level 1 centers do better with particularly nasty injuries (severe liver trauma, aortic, vena cava, iliac vascular, and penetrating cardiac injuries). However level 1 centers are hard to come by. Viewing the listing here, one notices the absence of verified ACS trauma centers of ANY level in Alabama, Florida, Georgia, South Carolina, or Tennessee.
Currently in Georgia legislature is forming a study committee to work on establishing a statewide trauma network. Safe America has launched an awareness program that includes public service announcements
Labels: Practice Makes Perfect
|![]()





