Tuesday, September 27, 2005
Over 100,000 Served.....
In my paucity of posting I neglected to mention that I have crossed over the 100,000 visitor mark. Thanks for stopping by. The day job has just gotten in the way over the past few weeks. Hopefully things will slow down over the next week. |
In my paucity of posting I neglected to mention that I have crossed over the 100,000 visitor mark. Thanks for stopping by. The day job has just gotten in the way over the past few weeks. Hopefully things will slow down over the next week. |
Sunday, September 25, 2005

Georgia 23 Mississippi State 10
The inability to "finish the drill" in the red zone could make things problematic for the Dogs as they play in Knoxville in two weeks. |
Monday, September 12, 2005
Buy that Man a Wheelbarrow.....
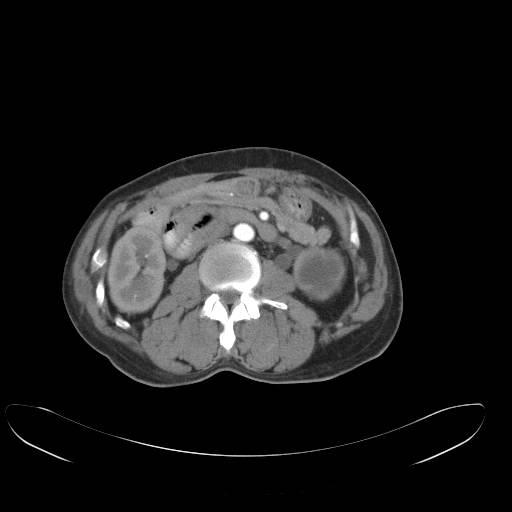
Haven't posted any pictures in awhile. 50-ish male admitted for back pain. His H&P actually said he was "sitting on his porch drinking as was his usual habit when he fell and hurt his back". I am asked to see him about a "hernia". He relates no signs or symptoms of incarceration and states it has been there for "a few months". I pull back the sheet and.....just say he made this guy look like an amateur.
Let's get a CT scan....

Not too bad right now.

Not a lot of bowel seen.....
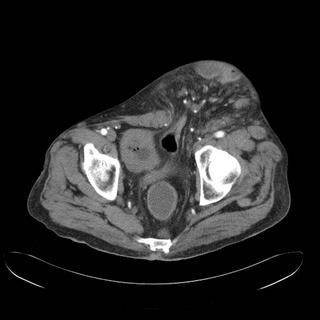
Here is the defect. About 8cm from my measurement.

Oh my. He seems to have more bowel in his scrotum than in his abdomen proper. This, to put it mildly, presents a problem. Given the size of the hernia just "shoving everything back in" really won't work. His abdomen has "gotten used" to the bowel not being there and he has what is called a "loss of domain". If the hernia was repaired in the usual fashion the chances of abdominal compartment syndrome and respiratory failure would be very high. In newborns with gastroschisis the treatment with a "silo" which covers the bowel and is eventually "rolled in" a little at the time to allow the abdomen to stretch. In adults it is not so easy. Papers have appeared that some centers are using "therapeutic pneumoperitoneum" to expand the abdominal cavity enough to allow for reduction of the contents. Having never done this I sent this fellow off to the Ivory Tower, where they have done this once or twice. |
Haven't posted any pictures in awhile. 50-ish male admitted for back pain. His H&P actually said he was "sitting on his porch drinking as was his usual habit when he fell and hurt his back". I am asked to see him about a "hernia". He relates no signs or symptoms of incarceration and states it has been there for "a few months". I pull back the sheet and.....just say he made this guy look like an amateur.
Let's get a CT scan....
Not too bad right now.

Not a lot of bowel seen.....

Here is the defect. About 8cm from my measurement.

Oh my. He seems to have more bowel in his scrotum than in his abdomen proper. This, to put it mildly, presents a problem. Given the size of the hernia just "shoving everything back in" really won't work. His abdomen has "gotten used" to the bowel not being there and he has what is called a "loss of domain". If the hernia was repaired in the usual fashion the chances of abdominal compartment syndrome and respiratory failure would be very high. In newborns with gastroschisis the treatment with a "silo" which covers the bowel and is eventually "rolled in" a little at the time to allow the abdomen to stretch. In adults it is not so easy. Papers have appeared that some centers are using "therapeutic pneumoperitoneum" to expand the abdominal cavity enough to allow for reduction of the contents. Having never done this I sent this fellow off to the Ivory Tower, where they have done this once or twice. |
Wednesday, September 07, 2005
Drunk versus Sleepy.....
From JAMA this week:Neurobehavioral Performance of Residents After Heavy Night Call vs After Alcohol Ingestion
The party:

Some problems with the study, as the authors point out:
I would also ask, given the study ended in August of 2003, is there enough power to determine if the reduction of hours (90 to 80) had any effect? Given the small numbers, probably not. Would be interesting to see this study repeated under the new limits. |
From JAMA this week:Neurobehavioral Performance of Residents After Heavy Night Call vs After Alcohol Ingestion
Context Concern exists about the effect of extended resident work hours; however, no study has evaluated training-related performance impairments against an accepted standard of functional impairment.The definition of "light" and "heavy" call were as follows:
Objectives To compare post-call performance during a heavy call rotation (every fourth or fifth night) to performance with a blood alcohol concentration of 0.04 to 0.05 g% (per 100 mL of blood) during a light call rotation, and to evaluate the association between self-assessed and actual performance.
Design, Setting, and Participants A prospective 2-session within-subject study of 34 pediatric residents (18 women and 16 men; mean age, 28.7 years) in an academic medical center conducted between October 2001 and August 2003, who were tested under 4 conditions: light call, light call with alcohol, heavy call, and heavy call with placebo.
Interventions Residents attended a test session during the final week of a light call rotation (non–post-call) and during the final week of a heavy call rotation (post-call). At each session, they underwent a 60-minute test battery (light and heavy call conditions), ingested either alcohol (light call with alcohol condition) or placebo (heavy call with placebo condition), and repeated the test battery. Performance self-evaluations followed each test.
Main Outcome Measures Sustained attention, vigilance, and simulated driving performance measures; and self-report sleepiness, performance, and effort measures.
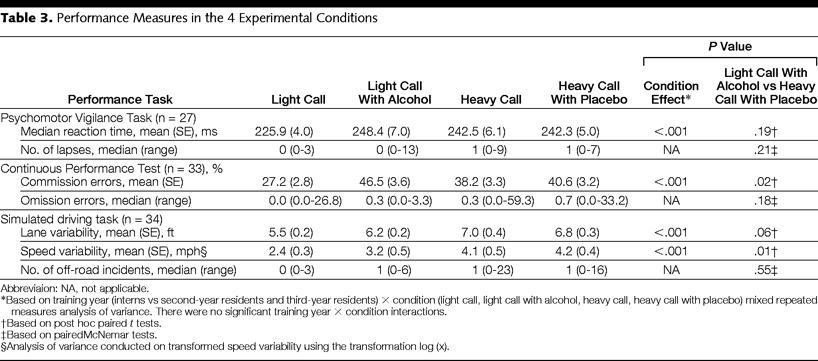
Results Participants achieved the target blood alcohol concentration. Compared with light call, heavy call reaction times were 7% slower (242.5 vs 225.9 milliseconds, P<.001); commission errors were 40% higher (38.2% vs 27.2%, P<.001); and lane variability (7.0 vs 5.5 ft, P<.001) and speed variability (4.1 vs 2.4 mph, P<.001) on the driving simulator were 27% and 71% greater, respectively. Speed variability was 29% greater in heavy call with placebo than light call with alcohol (4.2 vs 3.2 mph, P = .01), and reaction time, lapses, omission errors, and off-roads were not different. Correlation between self-assessed and actual performance under heavy call was significant for commission errors (r = –0.45, P = .01), lane variability (r = –0.76, P<.001), and speed variability (r = –0.71, P<.001), but not for reaction time.
Conclusions Post-call performance impairment during a heavy call rotation is comparable with impairment associated with a 0.04 to 0.05 g% blood alcohol concentration during a light call rotation, as measured by sustained attention, vigilance, and simulated driving tasks. Residents’ ability to judge this impairment may be limited and task-specific.
Light call rotations (behavioral, elective, or selective) were 4-week daytime clinic rotations averaging 44 hours per week, along with sick-call, which requires night call only if the on-call resident becomes ill. Heavy call rotations (neonatal intensive care, pediatric intensive care, or wards) averaged 90 hours per week (80 hours per week after July 2003) and mandated call every fourth or fifth night (34-36 consecutive hours per overnight call). Residents were allowed to work outside the authorized training program (moonlight) only with written permission from the residency director.
The party:
Following the light call condition testing, participants consumed alcohol (light call with alcohol condition). The alcohol dose was 0.6 g/kg for men and 0.55 g/kg for women, to produce equivalent peak BACs of 0.05 g%.42 The alcoholic beverage consisted of a commercial brand of chilled 80-proof vodka mixed with tonic water in a 1:5 ratio and one-fourth lime. Following the heavy call condition testing, participants consumed placebo (heavy call with placebo condition). The placebo was an equal volume of chilled tonic water and one-fourth lime. The total volume was distributed among three 12-oz cups and consumed at an equal rate over 30 minutes. To enhance the appearance that participants were receiving alcohol in both conditions, the drinks were mixed in plain view, alcohol and tonic were decanted from vodka bottles, and beverages were served with fresh lime.How tasty. The tabulated results:
Some problems with the study, as the authors point out:
Our study had several limitations. First, the small sample size meant that our main comparisons of interest had low statistical power, and we did not perform an intention-to-treat analysis. However, we successfully detected simulated driving differences between the heavy call with placebo and light call with alcohol groups and we had a relatively large sample size for studies on residents using a within-subjects design. We did not randomize or counterbalance the order of test conditions and cannot discount the possibility of order effects on our findings. However, the tests we used have relatively small practice effects41, 64-65 and all participants practiced the outcome measures before the first test session. In addition, secondary analyses, although underpowered, showed a similar pattern of results.
There may have been a self-selection bias, such that participants may have wanted to demonstrate worse impairment after heavy call than after alcohol ingestion, and our attempts to blind participants to the presence or absence of alcohol were frequently unsuccessful. However, we believe that these results are valid because we did not communicate our specific hypotheses to the participants, we found consistently worse light call with alcohol than light call performance, and effort ratings were higher in heavy call with placebo than light call with alcohol. It is unlikely that participants could have titrated their light call with alcohol performance to be systematically worse than light call but not worse than heavy call with placebo, or that they used greater effort in heavy call with placebo if the goal was to show worse heavy call with placebo than light call with alcohol impairment. Intentional poor performance in heavy call with placebo would have been achieved by exerting minimal effort on the tasks.
Although the tests selected for our study were carefully chosen surrogates for skills that we hypothesized would be impaired by sleep loss in medical residents, we are unable to draw firm conclusions about the degree of training-related impairment associated with actual medical tasks or medical decision making. Our findings do suggest, however, that some of the constituent skills necessary to perform medical tasks are likely to be impaired post-call during a typical heavy call rotation. Finally, our results may not generalize to subspecialties other than pediatrics or to other residency programs with different light and heavy call rotation schedules.
I would also ask, given the study ended in August of 2003, is there enough power to determine if the reduction of hours (90 to 80) had any effect? Given the small numbers, probably not. Would be interesting to see this study repeated under the new limits. |
Sunday, September 04, 2005
Georgia 48 Boise State 13
Georgia shuts out the top scoring offense in the NCAA 3 of the past 5 years for 38 minutes of football. Were the Broncos over-hyped? Perhaps.
Next week the most hated man in Georgia, Steve Spurrier, comes to Athens. |
![]()




