Saturday, July 30, 2005
When You Care Enough to Send the Very Best......

My mom sent me this, not often one sees a surgeon on the front of a greeting card. With school starting in two weeks My family and I are off to the beach. No medical reading, but I hope to finish reading Summer for the Gods (recently discussed at The Volokh Conspiracy). Hope to start and finish 1776, The Secret Man and try to get into Running the World. Optimistic, I'm sure but with no computer I'll have plenty of time. |

My mom sent me this, not often one sees a surgeon on the front of a greeting card. With school starting in two weeks My family and I are off to the beach. No medical reading, but I hope to finish reading Summer for the Gods (recently discussed at The Volokh Conspiracy). Hope to start and finish 1776, The Secret Man and try to get into Running the World. Optimistic, I'm sure but with no computer I'll have plenty of time. |
Thursday, July 28, 2005
Tales from the Trauma Service XII.......
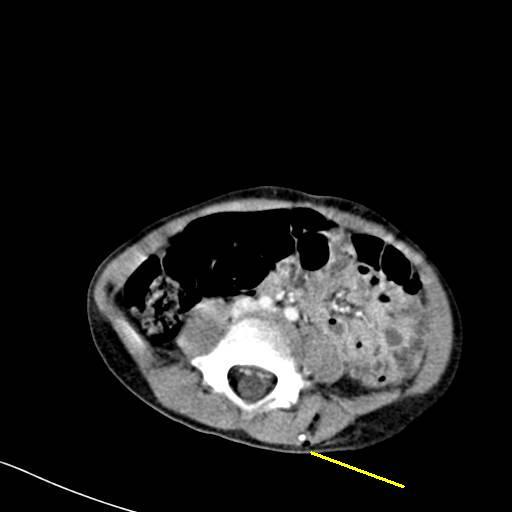
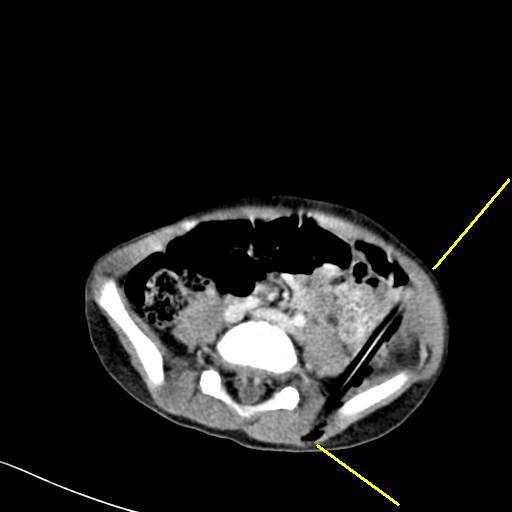
One of my partner's cases. Young man falls from a bunk bed and stikes a pencil that is part of an art project. Pictures are worth a thousand words they say:




The yellow lines represent the ends of the pencil.
The point was visible beneath the skin anteriorly. The youngster was taken to the OR for exploration and luckily missed everything. The ureter, iliac artery, and colon were uninjured.
Truth is stranger than fiction.
One of my partner's cases. Young man falls from a bunk bed and stikes a pencil that is part of an art project. Pictures are worth a thousand words they say:


The yellow lines represent the ends of the pencil.
The point was visible beneath the skin anteriorly. The youngster was taken to the OR for exploration and luckily missed everything. The ureter, iliac artery, and colon were uninjured.
Truth is stranger than fiction.
Labels: Tales from the Trauma Service
|Wednesday, July 27, 2005
Tales from the Operating Room VII....
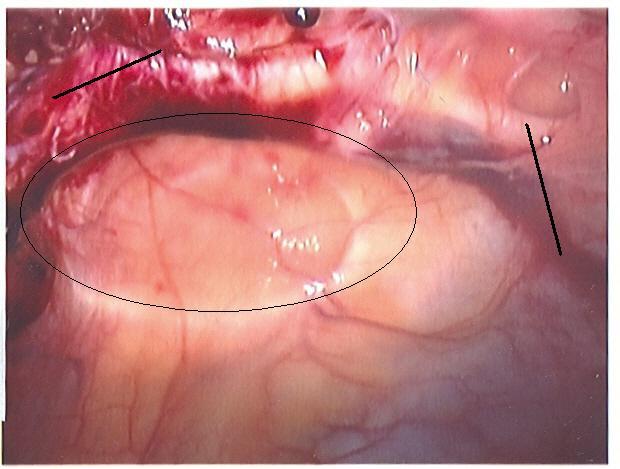
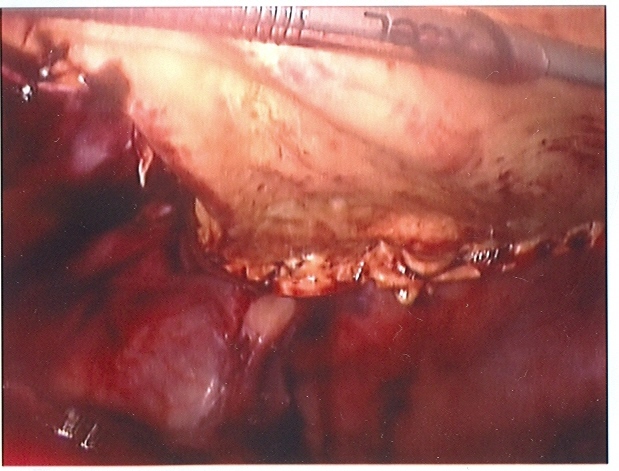
It has been awhile since I had pictures to post. 60-ish year old about 15 months out from a right hemicolectomy for a large polyp. Presented to me with about 2-3 months of abdominal "bulging". Exam revealed a hernia with approximately 6cm defect and a questionable defect superior to that one. To the OR:

The circle is the superiormost defect. It was the "questionable" one felt on physical exam.

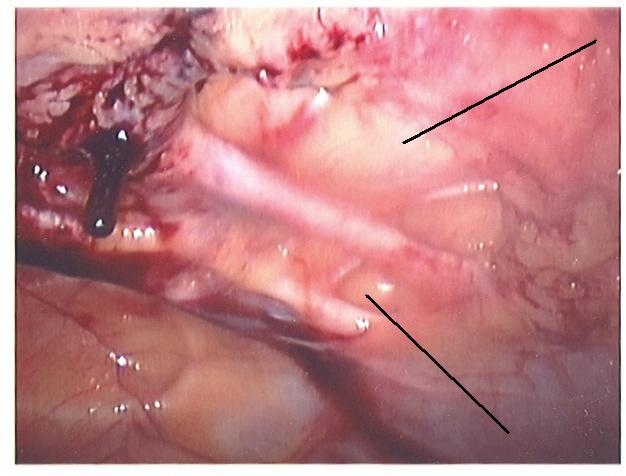
Working our way down, you can see the defect encircled above at the left.

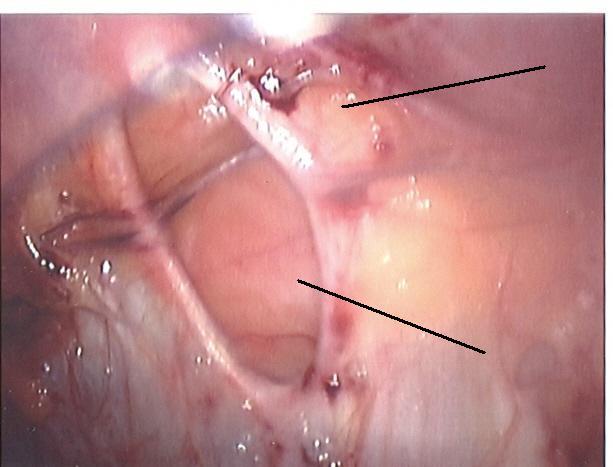
Some more.

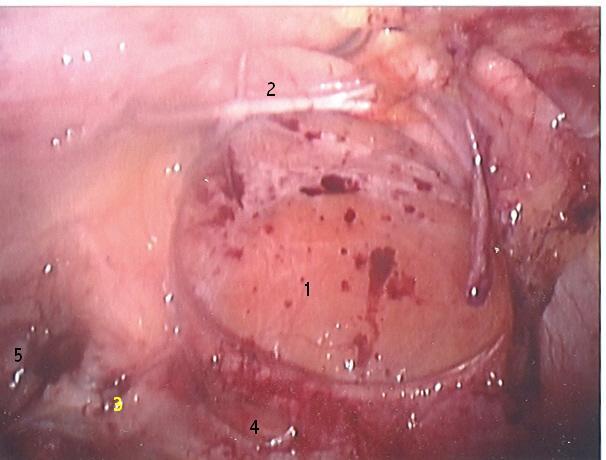
Five defects here. Defect number 1 was the palpable one that caused the patient to see me.
There were about 9 defects in all. The advantages of laparoscopic hernia repair can be summed up in these photos. Many of the smaller could have easily escaped detection during an anterior repair. Likely they would have increased in size and the patient would have presented with a "recurrence". This required a 32x18 cm sheet of Gore DualMesh to repair. Eight anchoring sutures were placed after numbering them and the mesh was placed into the abdomen. They sutures were brought through the abdominal wall with a Gore Suture Passer and tied. The mesh was then tacked to the anterior abdominal wall.
Here are the "after" pictures:




Technology can be wonderful. |
It has been awhile since I had pictures to post. 60-ish year old about 15 months out from a right hemicolectomy for a large polyp. Presented to me with about 2-3 months of abdominal "bulging". Exam revealed a hernia with approximately 6cm defect and a questionable defect superior to that one. To the OR:
The circle is the superiormost defect. It was the "questionable" one felt on physical exam.
Working our way down, you can see the defect encircled above at the left.
Some more.
Five defects here. Defect number 1 was the palpable one that caused the patient to see me.
There were about 9 defects in all. The advantages of laparoscopic hernia repair can be summed up in these photos. Many of the smaller could have easily escaped detection during an anterior repair. Likely they would have increased in size and the patient would have presented with a "recurrence". This required a 32x18 cm sheet of Gore DualMesh to repair. Eight anchoring sutures were placed after numbering them and the mesh was placed into the abdomen. They sutures were brought through the abdominal wall with a Gore Suture Passer and tied. The mesh was then tacked to the anterior abdominal wall.
Here are the "after" pictures:



Technology can be wonderful. |
Tuesday, July 26, 2005
Forbes on Medblogs.....
Forbes.com has review of some medblogs they consider the "best of the web". In addition to yours truly they review Family Medicine Notes, In the Pipeline, Medicine and Man, Medlogs, Medpundit, Codeblog,and Dr. Pho's newest endeavor: Straightfromthedoc.
Always nice to see our neighborhood getting wider exposure. |
Forbes.com has review of some medblogs they consider the "best of the web". In addition to yours truly they review Family Medicine Notes, In the Pipeline, Medicine and Man, Medlogs, Medpundit, Codeblog,and Dr. Pho's newest endeavor: Straightfromthedoc.
Always nice to see our neighborhood getting wider exposure. |
Grand Rounds XLIV
Phayngula asks "What do medbloggers do?" Other than sit in front of their computer and rant all day?. |
Phayngula asks "What do medbloggers do?" Other than sit in front of their computer and rant all day?. |
Monday, July 25, 2005
Seventh Edition......
Spent last Thursday and Friday in the triennial exercise of teaching ATLS. There is a new edition out with changes to both the content and presentation. The emphasis is on the "interaction" of the audience. Many slides are framed to start with open-ended questions: "What are some methods for controlling the airway?" The audience is then to provide some answers and the instructor uncovers the answer on the slide.
The leap of technology that has made this possible is the conversion of the program content to a PowerPoint format. This allows the use of fancy transitions and shading during the presentation. This works well....if the students read the book beforehand, not a guaranteed situation. So you will often get some off-the-wall answers, and inevitably some student will want to debate you over them.
The ACS has also taken great steps to protect their PowerPoint presentations. Ideally I would like to copy the disks to allow the instructors to have their own copies. But due to the rather tight protections placed on the disks I must send the original to the instructor from the set that costs $100. Apparently there was massive misappropriation of the slides in the past.
Overall, though, the changes are probably for the better, at least the students who were retaking the course thought so. |
Spent last Thursday and Friday in the triennial exercise of teaching ATLS. There is a new edition out with changes to both the content and presentation. The emphasis is on the "interaction" of the audience. Many slides are framed to start with open-ended questions: "What are some methods for controlling the airway?" The audience is then to provide some answers and the instructor uncovers the answer on the slide.
The leap of technology that has made this possible is the conversion of the program content to a PowerPoint format. This allows the use of fancy transitions and shading during the presentation. This works well....if the students read the book beforehand, not a guaranteed situation. So you will often get some off-the-wall answers, and inevitably some student will want to debate you over them.
The ACS has also taken great steps to protect their PowerPoint presentations. Ideally I would like to copy the disks to allow the instructors to have their own copies. But due to the rather tight protections placed on the disks I must send the original to the instructor from the set that costs $100. Apparently there was massive misappropriation of the slides in the past.
Overall, though, the changes are probably for the better, at least the students who were retaking the course thought so. |
Wednesday, July 20, 2005
Help The Doctor.....
I am looking into a PDA/phone combination and am debating the Treo 650 and the Samsung 730i. Anyone have suggestions? I would be grateful for any advice. |
I am looking into a PDA/phone combination and am debating the Treo 650 and the Samsung 730i. Anyone have suggestions? I would be grateful for any advice. |
Tuesday, July 19, 2005
Under the Knife......
Grand Rounds Forty-Three has block time today with my Rocky Mountain colleague Aggrivated DocSurg. |
Grand Rounds Forty-Three has block time today with my Rocky Mountain colleague Aggrivated DocSurg. |
Saturday, July 16, 2005
Self-Discovery Through Internet Personality Quizzes....

Elrond
A stern yet benevolent organizer who often knows best, your wits are keenly fixed on aiding efforts you deem worthy.
Now at this last we must take a hard road, a road unforeseen. There lies our hope, if hope it be. To walk into peril to Mordor.
Elrond is a character in the Middle-Earth universe. TheOneRing.net has a short biography.
Link via Powerline |
Elrond
A stern yet benevolent organizer who often knows best, your wits are keenly fixed on aiding efforts you deem worthy.
Now at this last we must take a hard road, a road unforeseen. There lies our hope, if hope it be. To walk into peril to Mordor.
Elrond is a character in the Middle-Earth universe. TheOneRing.net has a short biography.
Link via Powerline |
Inquiring Minds Want to Know......
In a comment to this post Azygos left this comment:
Another:
If you are having your procedure at an ambulatory surgery center (ASC):
Continuing:
If having a laparoscopic procedure:
I'm sure there are more questions you may think of, feel free to post them in the comments. |
In a comment to this post Azygos left this comment:
I realize this topic could be an entire post but what questions would you ask a surgeon before letting them operate on you?Some I have thought of:
Are you currently board certified?This assures that your surgeon has completed an accredited residency program and has undergone both written and oral examinations. The American Board of Surgery currently requires recertification every ten years. The ABS is moving to a "maintenance of certification" (MOC) program (see page 4) as the internal medicine board has done.
Another:
How many of (insert procedure here) have you done? How many have you done in the past year? Month?With the increasing body of evidence that surgeon and hospital volume are very important predictors of complications, or the lack thereof. You not only need to ascertain total experience, but also make sure that the last time your surgeon did this operation was during the Bush 41 administration.
If you are having your procedure at an ambulatory surgery center (ASC):
What provisions are made for complications at the surgery center?While most of the procedures performed at ASC's are simple and complications are rare, sometimes they can happen. You should make sure that plans for transfer to a full-service hospital are in place should you need it.
Continuing:
If I have a question or a problem at night or on the weekend who will be there to assist me?Your surgeon may take calls on his own patients at all times or may participate in a call group on nights and weekends. In a group practice you may deal with whoever is on call. Every surgeon has his or her own way of doing things and one is not necessarily right or wrong, but you should know how things will be done.
If having a laparoscopic procedure:
How often do you have to convert to an open procedure? How many of the open procedures have you done?The latter question is the more important of the two. The goal of any operation is to accomplish the goal (removing the gallbladder, repairing the hernia) in the safest way possible. The benefits provided by laparoscopy come in a distant second. A surgeon who tells you he "never" has to convert is either a liar or engages in very risky operative behavior, IMHO. Even the laparoscopic "gurus" have to open from time to time.
I'm sure there are more questions you may think of, feel free to post them in the comments. |
Tuesday, July 12, 2005
Free Air isn't Cheap Either......
Continuing with the free air theme I present this case from my just completed weekend on call.
Elderly gentleman with a long history of "stomach problems". He has been admitted several times in the past with obstipation. Colonoscopy has been attempted in the past but the scope kept "coiling up" in his sigmoid colon. He presented to the hospital with increasing abdominal pain and distension which according to his family physician is how he usually presents with his obstipation. On exam he was afebrile and did not appear ill. His abdomen was distended and had mild diffuse tenderness. His WBC count was mildly elevated but he did not have a left shift. A not too impressive set of facts until I saw this:

The yellow lines indicate the diaphragm with air underneath it.
So we have what appears to be a perforated viscus.
Most likely a perforated ulcer or a portion of colon. Given his history I am inclined to believe the latter.
So what to do? The patient's physical exam and lab workup is not as impressive as that xray. But given his age he may not manifest a leukocytosis or have guarding or rebound on physical exam. On one hand he would be at very high risk for postoperative complications and prolonged vent dependence, something neither he nor his family want. If it was a colonic perforation the probability of colostomy was close to 100 percent and given his age and medical problems would likely be a permanent one. Non-operative treatment with bowel rest and antibiotics could also be tried. But the patients at most risk for surgery are the same ones that would not tolerate decompensation during non-operative therapy. After extensive discussions with his family and primary physician the decision was made to proceed to the operating room.
The findings: 1)No evidence of perforation. No enteric contents within abdomen.
2)Massively dilated stomach with about 3000cc of gastric contents and air within the stomach.
3)Redundant colon without mass
4) Several small bowel adhesions without evidence of complete obstruction. Some loops are large
5)Atrophic left lobe of liver.
In other words, pretty much a negative exploration. There is a phenomenon known as Chilaiditi's Sign. Although this sign is primarily associated with colonic interposition, cases involving small bowel are mentioned as well. Fortunately he is doing well and will be discharged soon. |
Continuing with the free air theme I present this case from my just completed weekend on call.
Elderly gentleman with a long history of "stomach problems". He has been admitted several times in the past with obstipation. Colonoscopy has been attempted in the past but the scope kept "coiling up" in his sigmoid colon. He presented to the hospital with increasing abdominal pain and distension which according to his family physician is how he usually presents with his obstipation. On exam he was afebrile and did not appear ill. His abdomen was distended and had mild diffuse tenderness. His WBC count was mildly elevated but he did not have a left shift. A not too impressive set of facts until I saw this:

The yellow lines indicate the diaphragm with air underneath it.
So we have what appears to be a perforated viscus.
Most likely a perforated ulcer or a portion of colon. Given his history I am inclined to believe the latter.
So what to do? The patient's physical exam and lab workup is not as impressive as that xray. But given his age he may not manifest a leukocytosis or have guarding or rebound on physical exam. On one hand he would be at very high risk for postoperative complications and prolonged vent dependence, something neither he nor his family want. If it was a colonic perforation the probability of colostomy was close to 100 percent and given his age and medical problems would likely be a permanent one. Non-operative treatment with bowel rest and antibiotics could also be tried. But the patients at most risk for surgery are the same ones that would not tolerate decompensation during non-operative therapy. After extensive discussions with his family and primary physician the decision was made to proceed to the operating room.
The findings: 1)No evidence of perforation. No enteric contents within abdomen.
2)Massively dilated stomach with about 3000cc of gastric contents and air within the stomach.
3)Redundant colon without mass
4) Several small bowel adhesions without evidence of complete obstruction. Some loops are large
5)Atrophic left lobe of liver.
In other words, pretty much a negative exploration. There is a phenomenon known as Chilaiditi's Sign. Although this sign is primarily associated with colonic interposition, cases involving small bowel are mentioned as well. Fortunately he is doing well and will be discharged soon. |
Thursday, July 07, 2005
Fly the Union Jack Today....


"We shall fight on the beaches. We shall fight on the landing grounds. We shall fight in the fields, and in the streets, we shall fight in the hills. We shall never surrender!"-Winston Churchill |
Is Five Years Enough??????
From this month's Bulletin of the American College of Surgeons:How long Should Surgical Training Take?
From this month's Bulletin of the American College of Surgeons:How long Should Surgical Training Take?
The implementation of the 80-hour workweek in American residency programs has aroused significant debate within the surgical community regarding the length of surgical training. Currently, surgical residents have to be trained more efficiently in less time and are expected to provide perfect, error-free care once they graduate into the real world of surgical practice.This has gotten the powers that be thinking:
It is in this changing environment that some have questioned how long general surgery training should take. As the clinical experience obtained by residents decreases with the 80-hour workweek, it has been suggested that the traditional five years of residency are too few to create proficient surgeons, and that additional years of training are necessary. But in reality, is five the magic number of years required to learn the art of surgery? Experience garnered through decades of training general surgery residents tells us that it is. Yet, from a purely technical standpoint, how many cases does one really need to perform to be proficient? Defining mandatory basic skills is difficult because a surgeon is more than a technician. The development of a resident into a competent surgeon requires much more than just exposure to a certain number of cases.The number and type of cases is one of a few objective measurements than can be applied to residents. The other big ones are inservice scores and scores for written boards. The "fast track" programs are discussed:
How long this basic general surgery training should take varies according to subspecialty, with some requiring completion of a full five-year program before additional subspecialty training begins. Some people have challenged this approach, and the current standards required to enter certain subspecialties, such as plastic, cardiac, thoracic, vascular surgery, and others, may disappear in the future. Whether it is possible to learn surgical principles and technique regardless of the case is a subjective question. Likewise, how a general skill can be transferred into a specialty-specific skill varies according to the individual surgeon. But, do you need to be a Âsuper-pluri-potential general surgeon before going into a subspecialty? Is reduced training time for specialists a disaster waiting to happen? Are we weakening surgical training and sacrificing quality by letting all these changes happen?These are important questions since about 75% of residency graduates go on to fellowships.
Surgery cannot be compartmentalized; yet, for example, if your area of interest is breast surgery, do you really need to be proficient in trauma and transplantation? Is performing a pancreatectomy relevant to a plastic surgeon? Does a cardiac surgeon need formal training in colorectal surgery?The short answer is "probably not". Given the evidence of volume and outcomes the cardiac surgeon is probably better served concentrating on bypass and valves after a few years. Pancreatectomys are so infrequent that it come close to a crime to allow someone who will never have to perform that procedure to steal it from someone who only might do it. The ABS, IMHO, has been slow to realize this, at least when I took the written boards. Lots of questions on head and neck, and "send the patient to your friendly neighborhood ENT" was not an option.
These questions present surgical educators with an enormous challenge as to how we deliver the necessary skills and knowledge to the next generation. Lowering standards to fit lifestyles is unacceptable, especially in an era of surgical quality improvement programs, possible pay-for-performance, the growing predominance of volume as an indicator of quality, and the persistent liability crisis. Inadequate training will initiate a domino effect that will yield significant consequences for the future of surgery.While studies have so far shown no reduction in cases after the 80 hour week was introduced, it is still early in the game and the number of cases may yet fall. Given the link between volume and outcome the number of cases performed during training becomes even more important. If the numbers fall, the powers that be may find it necessary to increase the residency to six years. Surgical residencies have the potential, based on surveys, to become more popular to the workweek restrictions. If the training is extended, that popularity may evaporate. It is probably inevitable that early specialization tracks will become more prevalent. |
Monday, July 04, 2005
Happy Birthday America!!!!!
The Declaration of Independence

Be careful with the fireworks! Don't be the star of "Tales From the Trauma Service". |
The Declaration of Independence
IN CONGRESS, July 4, 1776.
The unanimous Declaration of the thirteen united States of America,
When in the Course of human events, it becomes necessary for one people to dissolve the political bands which have connected them with another, and to assume among the powers of the earth, the separate and equal station to which the Laws of Nature and of Nature's God entitle them, a decent respect to the opinions of mankind requires that they should declare the causes which impel them to the separation.
We hold these truths to be self-evident, that all men are created equal, that they are endowed by their Creator with certain unalienable Rights, that among these are Life, Liberty and the pursuit of Happiness.--That to secure these rights, Governments are instituted among Men, deriving their just powers from the consent of the governed, --That whenever any Form of Government becomes destructive of these ends, it is the Right of the People to alter or to abolish it, and to institute new Government, laying its foundation on such principles and organizing its powers in such form, as to them shall seem most likely to effect their Safety and Happiness. Prudence, indeed, will dictate that Governments long established should not be changed for light and transient causes; and accordingly all experience hath shewn, that mankind are more disposed to suffer, while evils are sufferable, than to right themselves by abolishing the forms to which they are accustomed. But when a long train of abuses and usurpations, pursuing invariably the same Object evinces a design to reduce them under absolute Despotism, it is their right, it is their duty, to throw off such Government, and to provide new Guards for their future security.--Such has been the patient sufferance of these Colonies; and such is now the necessity which constrains them to alter their former Systems of Government. The history of the present King of Great Britain is a history of repeated injuries and usurpations, all having in direct object the establishment of an absolute Tyranny over these States. To prove this, let Facts be submitted to a candid world.
He has refused his Assent to Laws, the most wholesome and necessary for the public good.
He has forbidden his Governors to pass Laws of immediate and pressing importance, unless suspended in their operation till his Assent should be obtained; and when so suspended, he has utterly neglected to attend to them.
He has refused to pass other Laws for the accommodation of large districts of people, unless those people would relinquish the right of Representation in the Legislature, a right inestimable to them and formidable to tyrants only.
He has called together legislative bodies at places unusual, uncomfortable, and distant from the depository of their public Records, for the sole purpose of fatiguing them into compliance with his measures.
He has dissolved Representative Houses repeatedly, for opposing with manly firmness his invasions on the rights of the people.
He has refused for a long time, after such dissolutions, to cause others to be elected; whereby the Legislative powers, incapable of Annihilation, have returned to the People at large for their exercise; the State remaining in the mean time exposed to all the dangers of invasion from without, and convulsions within.
He has endeavoured to prevent the population of these States; for that purpose obstructing the Laws for Naturalization of Foreigners; refusing to pass others to encourage their migrations hither, and raising the conditions of new Appropriations of Lands.
He has obstructed the Administration of Justice, by refusing his Assent to Laws for establishing Judiciary powers.
He has made Judges dependent on his Will alone, for the tenure of their offices, and the amount and payment of their salaries.
He has erected a multitude of New Offices, and sent hither swarms of Officers to harrass our people, and eat out their substance.
He has kept among us, in times of peace, Standing Armies without the Consent of our legislatures.
He has affected to render the Military independent of and superior to the Civil power.
He has combined with others to subject us to a jurisdiction foreign to our constitution, and unacknowledged by our laws; giving his Assent to their Acts of pretended Legislation:
For Quartering large bodies of armed troops among us:
For protecting them, by a mock Trial, from punishment for any Murders which they should commit on the Inhabitants of these States:
For cutting off our Trade with all parts of the world:
For imposing Taxes on us without our Consent:
For depriving us in many cases, of the benefits of Trial by Jury:
For transporting us beyond Seas to be tried for pretended offences
For abolishing the free System of English Laws in a neighbouring Province, establishing therein an Arbitrary government, and enlarging its Boundaries so as to render it at once an example and fit instrument for introducing the same absolute rule into these Colonies:
For taking away our Charters, abolishing our most valuable Laws, and altering fundamentally the Forms of our Governments:
For suspending our own Legislatures, and declaring themselves invested with power to legislate for us in all cases whatsoever.
He has abdicated Government here, by declaring us out of his Protection and waging War against us.
He has plundered our seas, ravaged our Coasts, burnt our towns, and destroyed the lives of our people.
He is at this time transporting large Armies of foreign Mercenaries to compleat the works of death, desolation and tyranny, already begun with circumstances of Cruelty & perfidy scarcely paralleled in the most barbarous ages, and totally unworthy the Head of a civilized nation.
He has constrained our fellow Citizens taken Captive on the high Seas to bear Arms against their Country, to become the executioners of their friends and Brethren, or to fall themselves by their Hands.
He has excited domestic insurrections amongst us, and has endeavoured to bring on the inhabitants of our frontiers, the merciless Indian Savages, whose known rule of warfare, is an undistinguished destruction of all ages, sexes and conditions.
In every stage of these Oppressions We have Petitioned for Redress in the most humble terms: Our repeated Petitions have been answered only by repeated injury. A Prince whose character is thus marked by every act which may define a Tyrant, is unfit to be the ruler of a free people.
Nor have We been wanting in attentions to our Brittish brethren. We have warned them from time to time of attempts by their legislature to extend an unwarrantable jurisdiction over us. We have reminded them of the circumstances of our emigration and settlement here. We have appealed to their native justice and magnanimity, and we have conjured them by the ties of our common kindred to disavow these usurpations, which, would inevitably interrupt our connections and correspondence. They too have been deaf to the voice of justice and of consanguinity. We must, therefore, acquiesce in the necessity, which denounces our Separation, and hold them, as we hold the rest of mankind, Enemies in War, in Peace Friends.
We, therefore, the Representatives of the united States of America, in General Congress, Assembled, appealing to the Supreme Judge of the world for the rectitude of our intentions, do, in the Name, and by Authority of the good People of these Colonies, solemnly publish and declare, That these United Colonies are, and of Right ought to be Free and Independent States; that they are Absolved from all Allegiance to the British Crown, and that all political connection between them and the State of Great Britain, is and ought to be totally dissolved; and that as Free and Independent States, they have full Power to levy War, conclude Peace, contract Alliances, establish Commerce, and to do all other Acts and Things which Independent States may of right do. And for the support of this Declaration, with a firm reliance on the protection of divine Providence, we mutually pledge to each other our Lives, our Fortunes and our sacred Honor.
Be careful with the fireworks! Don't be the star of "Tales From the Trauma Service". |
Friday, July 01, 2005
Terrible Twos.......
I started this blog two years ago today, and it has provided endless entertainment during that time. First a thank you to all those who link to this humble site as well as those who visit.
Secondly a thank you to Dr. Genes. The "father" of Grand Rounds has probably done more than anyone to increase the exposure of our little corner of the blogosphere. He has certainly increased my traffic. The number and quality of medical blogs continues to increase at a steady rate. When I started I was the solitary surgeon blogger. Now Orac and the Aggravated one deliver a high grade product on a regular basis.
Despite the great pleasure I derive from this endeavor there have been times that I have considered hanging it up. It is conventional wisdom that if you keep blogging for a year then the chances of it sticking around are higher. But I have found this past year to be more of a struggle some times. But just when I'm ready to quit, I find something that catches my eye.
Thanks again and best of luck to the new housestaff!! |
I started this blog two years ago today, and it has provided endless entertainment during that time. First a thank you to all those who link to this humble site as well as those who visit.
Secondly a thank you to Dr. Genes. The "father" of Grand Rounds has probably done more than anyone to increase the exposure of our little corner of the blogosphere. He has certainly increased my traffic. The number and quality of medical blogs continues to increase at a steady rate. When I started I was the solitary surgeon blogger. Now Orac and the Aggravated one deliver a high grade product on a regular basis.
Despite the great pleasure I derive from this endeavor there have been times that I have considered hanging it up. It is conventional wisdom that if you keep blogging for a year then the chances of it sticking around are higher. But I have found this past year to be more of a struggle some times. But just when I'm ready to quit, I find something that catches my eye.
Thanks again and best of luck to the new housestaff!! |
![]()





