Tuesday, June 29, 2004
JULY SURPRISE....
Kevin and Mr. Hawkins beat me to the punch on this New York Times story on the old "stay away from the hospital in July" story. Turns out that it's mostly bunk:
But there are always exceptions:
Kevin and Mr. Hawkins beat me to the punch on this New York Times story on the old "stay away from the hospital in July" story. Turns out that it's mostly bunk:
Several studies in the past few years have searched in vain for the phenomenon. One of the largest , published in The Journal of General Internal Medicine in 2003, compared hospital deaths and lengths of stay from July to September to the rates for other months in teaching and nonteaching hospitals. The researchers, Drs. William A. Barry and Gary E. Rosenthal of the University of Iowa Hospitals and Clinics in Iowa City, reviewed the records of more than 48,000 patients admitted to intensive care units in 28 hospitals in Ohio from 1991 to 1997. They found no significant difference in mortality rates or lengths of stay in the July-through-September period.
Of course, the study looked at the outcomes of very sick patients who were treated in intensive care units, where one would expect the highest degree of supervision, possibly obscuring a July effect. Other studies, however, have also failed to find differences in mortality rates for hospitalized patients in July.
But there are always exceptions:
But there is one group for whom a kind of July phenomenon might exist - psychiatric patients.The author goes on to write that it was so bad at one program that the program director forbade any vacations during July. Oh the horror!!! When I was a resident (walking to work barefoot in ten feet of snow uphill both ways....) we couldn't take vacations in June or July. What kind of resident would think about asking for a vacation in July anyway? |
They are followed by residents in hospital clinics, usually for one or two years, and learn some time in the spring that they will have new psychiatrists in July. For many who have grown attached to their therapists, this can be more than just upsetting. It can be literally destabilizing.
A study at the Payne Whitney Clinic of New York-Presbyterian Hospital and published in Hospital and Community Psychiatry found a statistically significant increase in hospitalization rates in the three- month period after the resident changeover compared with other months.
POMP AND CIRCUMSTANCE....
The FP residency program at Big Hospital had their graduation ceremony a few days ago. Everyone looked nice dressed up and it was a pleasure to meet some of their families. The graduation speaker based his talk on the book All I Really Need to Know I Learned in Kindergarten. Nicely done. Some of the residents are fulfilling scholarship requirements and practicing in rural Georgia. One is remaining as a member of the faculty. One is joining the hospitalist group in town. Two have military commitments, one will remain stateside..and another will be heading to Iraq in a few weeks.
This particular resident and I did not get along all that well on a personal level, but he worked hard and took care of business. This resident told me,that from what he had been told, he would get the most use out of what my partners and I had taught him. I thanked him for that, and shook his hand.
"Wear your helmet and be careful," I told him.
"I will be," he reassured me.
He will be in my thoughts and prayers
UPDATE: Goes to show what happens when you post in-between patients. I posted this before I was finished.
The ceremony was quiet and dignified...as opposed to some of the graduation ceremonies where I trained. An open bar can do that to a party. We also had roasts of the graduating residents. Not many parents came to our graduation ceremony so the roasts were, shall I say, not safe for work. One year a resident graduated who had done a great deal to earn some scalding...and his parents came. Not only did he and his parents have to endure the overtly risque' points but they would ask him about all of the inside jokes.
Needless to say I didn't invite my parents... |
The FP residency program at Big Hospital had their graduation ceremony a few days ago. Everyone looked nice dressed up and it was a pleasure to meet some of their families. The graduation speaker based his talk on the book All I Really Need to Know I Learned in Kindergarten. Nicely done. Some of the residents are fulfilling scholarship requirements and practicing in rural Georgia. One is remaining as a member of the faculty. One is joining the hospitalist group in town. Two have military commitments, one will remain stateside..and another will be heading to Iraq in a few weeks.
This particular resident and I did not get along all that well on a personal level, but he worked hard and took care of business. This resident told me,that from what he had been told, he would get the most use out of what my partners and I had taught him. I thanked him for that, and shook his hand.
"Wear your helmet and be careful," I told him.
"I will be," he reassured me.
He will be in my thoughts and prayers
UPDATE: Goes to show what happens when you post in-between patients. I posted this before I was finished.
The ceremony was quiet and dignified...as opposed to some of the graduation ceremonies where I trained. An open bar can do that to a party. We also had roasts of the graduating residents. Not many parents came to our graduation ceremony so the roasts were, shall I say, not safe for work. One year a resident graduated who had done a great deal to earn some scalding...and his parents came. Not only did he and his parents have to endure the overtly risque' points but they would ask him about all of the inside jokes.
Needless to say I didn't invite my parents... |
Monday, June 28, 2004
GET OUT THE VOTE:
Lileks versus the party volunteer over at today's Bleat. Mr. Lileks describes a young lady who can read from the script very well but cannot defend the positions. Her final point is about Senator Kerrry's plan to repeal the Bush tax cuts. Mr. Lileks goes on to give what he calls "The Parable of the Stairs", essentially a tale of "trickle down" economics. She didn't take to well to that:
Why indeed?
|
Lileks versus the party volunteer over at today's Bleat. Mr. Lileks describes a young lady who can read from the script very well but cannot defend the positions. Her final point is about Senator Kerrry's plan to repeal the Bush tax cuts. Mr. Lileks goes on to give what he calls "The Parable of the Stairs", essentially a tale of "trickle down" economics. She didn't take to well to that:
“Well, it’s a philosophical difference,” she sniffed. She had pegged me as a form of life last seen clilcking the leash off a dog at Abu Ghraib. “I think the money should have gone straight to those people instead of trickling down.” Those last two words were said with an edge.(emphasis mine)
“But then I wouldn’t have hired them,” I said. “I wouldn’t have new steps. And they wouldn’t have done anything to get the money.”
“Well, what did you do?” she snapped.
“What do you mean?”
“Why should the government have given you the money in the first place?”
“They didn’t give it to me. They just took less of my money.”
That was the last straw. Now she was angry. And the truth came out:
“Well, why is it your money? I think it should be their money.”
Then she left.
And walked down the stairs. I let her go without charging a toll. It’s the philanthropist in me.
Why indeed?
|
PATIENTS BEHAVING BADLY....
I fired a patient the other day, something I rarely do but the behavior of him and his family really went beyond the pale.
This was a mid-30's man admitted with an emergent condition. While in the hospital he was found to have a DVT. It was in is common femoral system and had a free floating tail. He had severe contraindications to anticoagulation. I was asked to place a filter to protect him from a PE. I explained to his wife that this would not resolve the clot, and could even make any leg symptoms worse. She understood. Filter placed without difficulty. This was about six weeks ago.
A week or so ago they call my partner and tell him his leg is "swollen and blue". Since it is a Sunday he is directed to the ER. He is treated and released.
He follows-up with me a few days later. I review the ED note and find no reference to any cyanosis of his leg, although it is noted to be "slightly swollen". The exam at that time was consistent with the above. I speak to his other physician who thinks it is safe to start him on anticoagulation. He has limited funds and no insurance but is getting help from a local church with medical bills. I write prescriptions for low-molecular weight heparin (LMWH) and Coumadin. I instruct him to start the LMWH today and the Coumadin in about 2-3 days.
At the end of the encounter his wife starts asking questions about his home health and physical therapy arrangements. I ask her to discuss those issues with the physician who made those arrangements. She tells me that the home health people have told her that "any" of her husband's physicians can adjust them. I tell her that I will manage her husband's anticoagulation and his post-phlebitic syndrome, but those other issues need to be addressed by his other physician. All during this the patient, his wife, and another adult watch passively as a 10 year old child goes through drawers and disrupts pictures on the wall. I also order a venous duplex and a PT/INR for 5 days in the future and have them follow-up.
Two days later his wife calls, demanding that his home health orders be adjusted. My staff explains again that those issues need to be brought up with his other physician. The patient's wife becomes verbally abusive with the staff and uses a racial slur to describe the staff member she is talking with.
The dismissal letter went out that day.
I can empathize with their situation. I was treating this patient for free and without any expectation of future reimbursement. I'm a physician, that is what I do. I don't even expect a "thank you". But I will not put up with outright abuse of my staff. By anyone. Especially abuse such as described above. It's not worth it.
|
I fired a patient the other day, something I rarely do but the behavior of him and his family really went beyond the pale.
This was a mid-30's man admitted with an emergent condition. While in the hospital he was found to have a DVT. It was in is common femoral system and had a free floating tail. He had severe contraindications to anticoagulation. I was asked to place a filter to protect him from a PE. I explained to his wife that this would not resolve the clot, and could even make any leg symptoms worse. She understood. Filter placed without difficulty. This was about six weeks ago.
A week or so ago they call my partner and tell him his leg is "swollen and blue". Since it is a Sunday he is directed to the ER. He is treated and released.
He follows-up with me a few days later. I review the ED note and find no reference to any cyanosis of his leg, although it is noted to be "slightly swollen". The exam at that time was consistent with the above. I speak to his other physician who thinks it is safe to start him on anticoagulation. He has limited funds and no insurance but is getting help from a local church with medical bills. I write prescriptions for low-molecular weight heparin (LMWH) and Coumadin. I instruct him to start the LMWH today and the Coumadin in about 2-3 days.
At the end of the encounter his wife starts asking questions about his home health and physical therapy arrangements. I ask her to discuss those issues with the physician who made those arrangements. She tells me that the home health people have told her that "any" of her husband's physicians can adjust them. I tell her that I will manage her husband's anticoagulation and his post-phlebitic syndrome, but those other issues need to be addressed by his other physician. All during this the patient, his wife, and another adult watch passively as a 10 year old child goes through drawers and disrupts pictures on the wall. I also order a venous duplex and a PT/INR for 5 days in the future and have them follow-up.
Two days later his wife calls, demanding that his home health orders be adjusted. My staff explains again that those issues need to be brought up with his other physician. The patient's wife becomes verbally abusive with the staff and uses a racial slur to describe the staff member she is talking with.
The dismissal letter went out that day.
I can empathize with their situation. I was treating this patient for free and without any expectation of future reimbursement. I'm a physician, that is what I do. I don't even expect a "thank you". But I will not put up with outright abuse of my staff. By anyone. Especially abuse such as described above. It's not worth it.
|
LIEN ON ME....
From the Medical Association of Georgia:
Glad to see we got something out of the 2004 General Assembly session. |
From the Medical Association of Georgia:
As a result of MAG’s lobbying efforts, the General Assembly has passed a law, which will allow physicians to file a lien for their reasonable charges incurred in treating a patient who has suffered an injury and has filed a lawsuit as a result of that injury. The lien will be placed on any settlement of the lawsuit or a judgment after trial. Physicians should file the lien with the clerk of the superior court of the county in which the medical practice is located and in the county in which the patient resides along with a verified statement setting forth the name and address of the patient, the name and address of the medical practice, the dates of treatment and the amount of the charges. Previously, hospitals had the right to file such a lien but physicians did not. The bill will take effect on July 1, 2004.
Glad to see we got something out of the 2004 General Assembly session. |
Sunday, June 27, 2004
GO TO THE ER....
A little behind the curve here, but I wanted to comment on recent posts from Kevin MD and Medpundit on the use, misuse, and abuse of the emergency room. Reasons such as convenience, avoidance of referrals, multiple opinions, and inability to see one's own physician are given to explain this. While many visit the ER for things that can be evaluated at the office or clinic, acute abdominal pain is not one of them. Almost weekly my office fields a call from a physician's office wanting to send over someone with a "rule out appendicitis" problem. They get all worked-up when we ask they be sent to the emergency room. They complain about the wait, the crowds, ect.. I have to explain that while my office is pleasant and well equipped there are somethings we can't do:
Draw labs
Perform x-rays
Give IV fluids or pain medications
All of which are essential to evaluate a patient with acute abdominal pain. So if I see them in the office it's off to the ER anyway... |
A little behind the curve here, but I wanted to comment on recent posts from Kevin MD and Medpundit on the use, misuse, and abuse of the emergency room. Reasons such as convenience, avoidance of referrals, multiple opinions, and inability to see one's own physician are given to explain this. While many visit the ER for things that can be evaluated at the office or clinic, acute abdominal pain is not one of them. Almost weekly my office fields a call from a physician's office wanting to send over someone with a "rule out appendicitis" problem. They get all worked-up when we ask they be sent to the emergency room. They complain about the wait, the crowds, ect.. I have to explain that while my office is pleasant and well equipped there are somethings we can't do:
Draw labs
Perform x-rays
Give IV fluids or pain medications
All of which are essential to evaluate a patient with acute abdominal pain. So if I see them in the office it's off to the ER anyway... |
WHY TRAUMA SURGEONS LOVE ULTRASOUND....

Posted by Hello
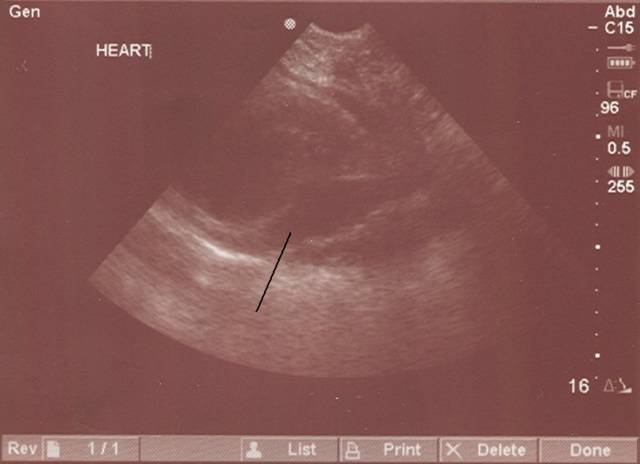
29 Y/O with a stab wound medial and inferior to left nipple. Hypotensive. Minimal response to fluids. Image is pericardial view obtained with a SonoSite Titan machine. Black line indicates fluid within pericardial sac. Taken to OR and explored with release of tamponade. 3mm wound on anterior right ventricle which was no longer actively bleeding. Pericardium left open and left chest tube placed. Pretty cool. |
Posted by Hello
29 Y/O with a stab wound medial and inferior to left nipple. Hypotensive. Minimal response to fluids. Image is pericardial view obtained with a SonoSite Titan machine. Black line indicates fluid within pericardial sac. Taken to OR and explored with release of tamponade. 3mm wound on anterior right ventricle which was no longer actively bleeding. Pericardium left open and left chest tube placed. Pretty cool. |
Saturday, June 26, 2004
MY OWN BILLING WOES.....
Jacob tells a tale of spending 90 minutes on his day off on the phone attempting to get $59 worth of reimbursement. All because he used a "mental health" ICD-9 code. The ICD/CPT coding system is complex and difficult to use, especially in the evaluation and management arena. What separates a high-complexity initial inpatient visit versus a moderate one? Even the experts have difficulty reaching agreement. As surgeon, however, I have many problems with the procedural codes (10021-75996). That is about 250 pages in the 2004 CPT guide. There are many procedures that have been performed for several years (laparoscopic ventral herniorraphy and laparoscopic colectomies) that have no specific CPT codes. If, for example, I perform a laparoscopic ventral hernia, and use CPT 49659 (Unlisted laparoscopy procedure, hernioplasty, herniorrhaphy,herniotomy), the claim will be denied. So the open repair code (49560) and mesh implantation (49568)is used, and this usually insures payment. Payment for supervision of conscious sedation (99141), used when attempting to reduce a hernia, is frequently denied. The basis is that I am not an anesthesiologist. The use of ultrasound in the evaluation of the trauma patient is widely accepted. Yet my submission of the code for a FAST exam (76705) is routinely denied. I guess they would rather pay thousands for a CT scan.
My partner attends coding conferences where he is told that insurance companies will not open their mail on Thursday or Friday on the oft chance that a claim will lapse. Medicare and Medicaid a often no better, as the last two examples above were Medicare/Medicaid denials. Much like Jacob, my practice writes off thousands of dollars. Payers deny claims because they know that not every physician is going to take the time, or go through the effort, to collect that fifty-nine dollars. |
Jacob tells a tale of spending 90 minutes on his day off on the phone attempting to get $59 worth of reimbursement. All because he used a "mental health" ICD-9 code. The ICD/CPT coding system is complex and difficult to use, especially in the evaluation and management arena. What separates a high-complexity initial inpatient visit versus a moderate one? Even the experts have difficulty reaching agreement. As surgeon, however, I have many problems with the procedural codes (10021-75996). That is about 250 pages in the 2004 CPT guide. There are many procedures that have been performed for several years (laparoscopic ventral herniorraphy and laparoscopic colectomies) that have no specific CPT codes. If, for example, I perform a laparoscopic ventral hernia, and use CPT 49659 (Unlisted laparoscopy procedure, hernioplasty, herniorrhaphy,herniotomy), the claim will be denied. So the open repair code (49560) and mesh implantation (49568)is used, and this usually insures payment. Payment for supervision of conscious sedation (99141), used when attempting to reduce a hernia, is frequently denied. The basis is that I am not an anesthesiologist. The use of ultrasound in the evaluation of the trauma patient is widely accepted. Yet my submission of the code for a FAST exam (76705) is routinely denied. I guess they would rather pay thousands for a CT scan.
My partner attends coding conferences where he is told that insurance companies will not open their mail on Thursday or Friday on the oft chance that a claim will lapse. Medicare and Medicaid a often no better, as the last two examples above were Medicare/Medicaid denials. Much like Jacob, my practice writes off thousands of dollars. Payers deny claims because they know that not every physician is going to take the time, or go through the effort, to collect that fifty-nine dollars. |
YOU CAN'T TAKE IT WITH YOU...
More entertainment courtesy of Georgia Medicaid. First look at this from the Atlanta Journal-Constitution:
Families denounce plans for Medicaid
I can't imagine what the hue and cry would be if Georgia was the first state to try and do this. I could point out the selfishness of those quoted above but Neal Boortz gave a no-holds barred rant on his site yesterday.
Oh man ... you should hear the wailing and gnashing of teeth going on over this plan. Ruby's children asked if state officials were "going to bear down this hard on our elderly population and go for the jugular vein?" Hey, kids. The taxpayers have been forking over big bucks for a few years not to take care of your mother. Where were you then? Were you whining about the state using its police power to seize money from people you don't even know to pay for your mother's nursing home care? Does it occur to you that these people had something else they could be spending that money for? Maybe they had medical expenses in their own family that needed to be covered. Maybe they were behind on their mortgage, or needed repairs to their car. Did that bother you? No, you just stood by and watched the state use its police power to seize money from complete strangers to care for your mother. I sure would be interested to find out just how much you two were willing to dip into your savings to pay for your mother's medical care. But hell, why should you? Why even bother when the state will take care of it all for you!....We all know what the deal here is, don't we? Ruby Fair's kids will get those 162 acres once she gets tucked in for that eternal celestial dirt nap. Now the state is threatening to take that land, sell it, and reimburse the people who have been taking care of Ruby Fair while her children dreamed of inheritances.....Then we have William Morris. He's quoted in the article also. His wife's uncle is in a Fairburn nursing home at state expense. Evidently the wife's uncle has some assets that the state is eyeing. William Morris says "this is theft ... hard-core theft." Pray tell, Mr. Morris, what is it when the government takes money away from me to pay for your relative's nursing home stay? Let me see if I get this straight: You take money from me to pay for your wife's uncle's medical care, no problem. You make your uncle pay the costs of his own care and that's theft......The run isn't over. We also have William Pinkney. His parents are both in a taxpayer-funded community health services program. Pinkney says that it was his father's dream to leave his property to his children and grandchildren. "Unfortunately with this proposal, their American dream just went away." OK .. now let me get this straight. Your version of the American dream is to use the police power of government to force other people to pay medical bills for your parents so that their estate will remain intact for you to inherit when they die. Fascinating.
The regulations may be found here. Some highlights:
So it doesn't seem that when you die your heirs will be hit with a bill for all of your Medicaid charges, only some of them. And there are some limitations:
The state may also place a lien on your property:
But they may not be enforceable:
There are even hardship provisions:
None of the family members quoted above are threatened with the loss of their own homes or businesses because of this. The question may be asked, should these families lose their assets, acquired over a lifetime of hard work, to pay for their medical care? There are plenty of people who do not own homes or large tracts of land who pay the taxes that fund the Medicaid program. Is it fair for them to have subsidized their medical care while the heirs enjoy the inheritance? If the eligibility criteria for Medicaid used assets instead of income, the system would be fairer. Now this could lead to property or other assets being sold to heirs for pennies on the dollar, but "Medicaid Planning" is nothing new.
This is a very controversial issue, and will probably grow in scope as healthcare funding becomes more scarce. Let the debate begin. |
More entertainment courtesy of Georgia Medicaid. First look at this from the Atlanta Journal-Constitution:
Families denounce plans for Medicaid
Ruby Fair, 91, resides in a Louisville nursing home, with her care paid for since 2001 by the state's Medicaid program for the poor and disabled.
The 162 acres she inherited in Louisville, in east Georgia, is the only thing she owns of value. But that former farmland in her family for decades may go to the state under a new program that seeks to recover the state's costs for delivering long-term care. Fair's son Roy and her daughter Pat Lamb were among family members and advocates for the elderly who testified Thursday at a state Department of Community Health public hearing on Georgia's plan to go after the homes and other assets of people receiving long-term care under Medicaid. The program starts in August.
"Are they going to bear down this hard on our elderly population and go for the jugular vein?'' Lamb said.
The General Assembly approved "estate recovery," part of Gov. Sonny Perdue's budget plan for the upcoming fiscal year. State officials have said that a tight budget forced them to take the action, which is required by federal law. Georgia is one of the last states in the nation to recover Medicaid costs this way.
"This is theft . . . hard-core theft,'' said William Morris, whose wife's uncle is in a Fairburn nursing home. "Something needs to be done about this.''
Many were angry that those already receiving long-term care would not be exempted from the rule change. The state plans to seek costs dating back to August 2001.
Seeking repayment for services provided before the rule was changed "is unconstitutional,'' said Joy Shirley of Newnan, whose father died in a nursing home earlier this year. She said the family was told during his stay it wouldn't have to repay the costs. "We were misled,'' Shirley said.
The state also plans to eliminate a program that helps pay for nursing home care for about 1,700 people considered "medically needy'' making too much income to qualify for Medicaid, but not enough to afford private nursing home rates.
Under estate recovery, Georgia will seek repayment of Medicaid benefits received by people 55 and older, as well as younger recipients who lived in a nursing home or other institutions for at least six months.
Georgia officials say they expect to collect $5 million the first year from the estates of Medicaid recipients.
About 39,000 Georgians age 55 and older in a year receive nursing home coverage through Medicaid, which covers 1.4 million low-income residents in the state. The changes will also affect an additional 15,000 Georgians in that age group who receive other types of Medicaid long-term care community or home-based services.
William Pinkney's parents both receive Medicaid-funded community services.
Pinkney said his mother, 85, has Alzheimer's disease, and his father, 92, has congestive heart failure. They need the state's assistance, he said, to remain in their Atlanta home and out of a nursing home, which would cost the state much more.
"I've been serving,'' said Pinkney, referring to his 27-year career in the military, now with Air National Guard. "It's about time the state started to serve me.''
He said it was his father's dream to leave his property for his children and grandchildren. "Unfortunately with this proposal, their American dream just went away.''
I can't imagine what the hue and cry would be if Georgia was the first state to try and do this. I could point out the selfishness of those quoted above but Neal Boortz gave a no-holds barred rant on his site yesterday.
Oh man ... you should hear the wailing and gnashing of teeth going on over this plan. Ruby's children asked if state officials were "going to bear down this hard on our elderly population and go for the jugular vein?" Hey, kids. The taxpayers have been forking over big bucks for a few years not to take care of your mother. Where were you then? Were you whining about the state using its police power to seize money from people you don't even know to pay for your mother's nursing home care? Does it occur to you that these people had something else they could be spending that money for? Maybe they had medical expenses in their own family that needed to be covered. Maybe they were behind on their mortgage, or needed repairs to their car. Did that bother you? No, you just stood by and watched the state use its police power to seize money from complete strangers to care for your mother. I sure would be interested to find out just how much you two were willing to dip into your savings to pay for your mother's medical care. But hell, why should you? Why even bother when the state will take care of it all for you!....We all know what the deal here is, don't we? Ruby Fair's kids will get those 162 acres once she gets tucked in for that eternal celestial dirt nap. Now the state is threatening to take that land, sell it, and reimburse the people who have been taking care of Ruby Fair while her children dreamed of inheritances.....Then we have William Morris. He's quoted in the article also. His wife's uncle is in a Fairburn nursing home at state expense. Evidently the wife's uncle has some assets that the state is eyeing. William Morris says "this is theft ... hard-core theft." Pray tell, Mr. Morris, what is it when the government takes money away from me to pay for your relative's nursing home stay? Let me see if I get this straight: You take money from me to pay for your wife's uncle's medical care, no problem. You make your uncle pay the costs of his own care and that's theft......The run isn't over. We also have William Pinkney. His parents are both in a taxpayer-funded community health services program. Pinkney says that it was his father's dream to leave his property to his children and grandchildren. "Unfortunately with this proposal, their American dream just went away." OK .. now let me get this straight. Your version of the American dream is to use the police power of government to force other people to pay medical bills for your parents so that their estate will remain intact for you to inherit when they die. Fascinating.
The regulations may be found here. Some highlights:
(2) Recovery will be pursued from Medicaid members:
(a) Who at the time of death was any age and an inpatient in a nursing facility, intermediate care facility for the mentally retarded, or other mental institution if the individual is required, as a condition of receiving services in the facility under the state plan, to spend for costs of medical care all but a minimal amount of the persons income required for personal needs; or
(b) Who at the time of death were fifty-five (55) years of age or older when the individual received medical assistance, but only for medical services consisting of nursing facility services, personal care services, home and community based services, and hospital and prescription drug services provided to individuals in nursing facilities or receiving home and community based services.
So it doesn't seem that when you die your heirs will be hit with a bill for all of your Medicaid charges, only some of them. And there are some limitations:
(7) The debt created in this section shall not be enforced if the member is survived by:
(a) A spouse;
(b) A child or children under twenty-one (21) years of age; or
(c) A child or children who are blind or permanently and totally disabled pursuant to the eligibility requirements of Title XIX of the Social Security Act.
The state may also place a lien on your property:
(2) The state may place a lien on the members home when there is not a reasonable
expectation that the member will return home and when none of the following persons
are living in the home:
(a) The members spouse;
(b) A child under twenty-one (21) years of age;
(c) A disabled child of any age; or
(d) A sibling with an equity interest in the home who has lived in the home for at least one (1) year before the member entered the nursing home.
But they may not be enforceable:
(9) The state may not enforce a lien under any of the following circumstances:
(a) The members spouse is alive, even if not living in the home;
(b) The members child under twenty-one (21) years of age is alive, even if not living in the home;
(c) The members blind or disabled child of any age is alive, even if not living in the home;
(d) An adult child of the member is living in the home, if that child lived in the home for at least two (2) years prior to the members admission to the nursing home and provided care that kept the member from entering a nursing home.
(e) The members brother or sister is living in the home, if he or she lived in the home for at least two (2) years prior to the members admission to a nursing home.
There are even hardship provisions:
(4) Recovery will be waived of any estate recovery when the requesting party is able to show,through clear and convincing evidence, that the states pursuit of estate recovery subjects them to undue hardship. In determining whether an undue hardship exists, the following criteria will be used:
(a) The asset to be recovered is a income producing farm of one or more of the heirs and the annual gross income is limited to $25,000 or less; or
(b) The recovery of assets would result in the applicant becoming eligible for governmental public assistance based on need and/or medical assistance programs.
(5) Undue hardship does not exist when:
(a) The adjustment or recovery of the clients cost of assistance would merely cause the clients family members inconvenience or restrict the familys lifestyle;
(b) The heir divests assets to qualify under the hardship provision.
None of the family members quoted above are threatened with the loss of their own homes or businesses because of this. The question may be asked, should these families lose their assets, acquired over a lifetime of hard work, to pay for their medical care? There are plenty of people who do not own homes or large tracts of land who pay the taxes that fund the Medicaid program. Is it fair for them to have subsidized their medical care while the heirs enjoy the inheritance? If the eligibility criteria for Medicaid used assets instead of income, the system would be fairer. Now this could lead to property or other assets being sold to heirs for pennies on the dollar, but "Medicaid Planning" is nothing new.
This is a very controversial issue, and will probably grow in scope as healthcare funding becomes more scarce. Let the debate begin. |
Friday, June 25, 2004
SEEING IS BELIEVING....
Now that his site is new and improved Mr. Page takes a big swallow of the single-payer kool-aid with this story from the Atlanta Journal-Constitution
Sounds like a good idea. I would like to learn more about it, but I can't.
I have Googled Georgians for a Common Sense Health Plan, Healthcare Georgia Foundation, Lewin Group, and even Rita Valenti. None of those searches revealed any sort of link to this study. No mention of the methods used or how they came up with the figure of $716 million saved with such a system. Finaly using Georgia Secure Care I was able to learn of a meeting in Atlanta where it will be discussed. "Learn the details with us" is the tagline. One should not have to drive to Atlanta to do so.
No surprise of how it is funded:
So they plan to use sales taxes and excise taxes to finance this. Aren't these the same taxes that are criticized for their regressive nature?
Yet another plan modeled after Medicare. The last I read and heard, physicians were starting to steer away from Medicare because of lousy reimbursement and red tape. So why are plans modeled after an unpopular system? And to turn it over to a crowd that can't balance the books, follow the rules or restrain themselves from throwing money away. They will also kick granny out of the nursing home on short notice.
Such is the beauty of federalism that the states can experiment with such plans to find out which ones work. But if put to the voters of Georgia, believeve it would suffer the same fate as the 2002 Oregon referendum.
One of the most useful things that blogs and other online resources allow us to to is "fact check" a portion of the writer's anatomy. I have tried and cannot find any facts to check about Ms. Valenti's plan. If my readers have any I would appreciate them. |
Now that his site is new and improved Mr. Page takes a big swallow of the single-payer kool-aid with this story from the Atlanta Journal-Constitution
A proposal for a Medicare-like system that would give health insurance coverage to all Georgia residents would cut total health spending for the state by about $716 million annually, according to study released Monday by a consumer group.
The proposed, government-run "single-payer" plan would be financed by a combination of payroll taxes, increases in tobacco and alcohol taxes, a 1 percent sales tax and a tax on individuals, said Georgians for a Common Sense Health Plan, a group that promotes health coverage for all residents.
But all current payments by employers and individuals, including health insurance premiums and co-pays, would be eliminated under the consumer group's SecureCare program. Most families earning $75,000 or less would pay less under the proposal, said Rita Valenti, a registered nurse and former state legislator who's a founder of the Common Sense group.
"The need is growing exponentially'' for such a plan, Valenti said, citing the rising number of uninsured  1.2 million in Georgia  and increasing health costs for consumers.
The SecureCare proposal would replace the current employer-based benefits system. "Most people realize our health care system is broken,'' Valenti said.
The study, conducted by the Virginia-based Lewin Group, a health care consulting firm, was financed by a grant from the nonprofit Healthcare Georgia Foundation, a private organization whose mission, in part, is to expand access to affordable, quality health care.
The Lewin Group has done analyses of single-payer proposals in other states, including California. No state has adopted such a plan.
Sounds like a good idea. I would like to learn more about it, but I can't.
I have Googled Georgians for a Common Sense Health Plan, Healthcare Georgia Foundation, Lewin Group, and even Rita Valenti. None of those searches revealed any sort of link to this study. No mention of the methods used or how they came up with the figure of $716 million saved with such a system. Finaly using Georgia Secure Care I was able to learn of a meeting in Atlanta where it will be discussed. "Learn the details with us" is the tagline. One should not have to drive to Atlanta to do so.
No surprise of how it is funded:
....would be financed by a combination of payroll taxes, increases in tobacco and alcohol taxes, a 1 percent sales tax and a tax on individuals...
So they plan to use sales taxes and excise taxes to finance this. Aren't these the same taxes that are criticized for their regressive nature?
Yet another plan modeled after Medicare. The last I read and heard, physicians were starting to steer away from Medicare because of lousy reimbursement and red tape. So why are plans modeled after an unpopular system? And to turn it over to a crowd that can't balance the books, follow the rules or restrain themselves from throwing money away. They will also kick granny out of the nursing home on short notice.
Such is the beauty of federalism that the states can experiment with such plans to find out which ones work. But if put to the voters of Georgia, believeve it would suffer the same fate as the 2002 Oregon referendum.
One of the most useful things that blogs and other online resources allow us to to is "fact check" a portion of the writer's anatomy. I have tried and cannot find any facts to check about Ms. Valenti's plan. If my readers have any I would appreciate them. |
Wednesday, June 23, 2004
WHAT DO YOU MEAN "'LESION' IS NOT AN ADEQUATE HISTORY ON A PATHOLOGY REQUISITION"?
This reminds me of a joke:
I didn't say it was a funny joke... |
This reminds me of a joke:
An internist, a surgeon, and a pathologist are in a duck blind waiting for some birds. After awhile they hear a "Quack! Quack!". The internist stands and says, "That sounds like a duck, looks like a duck, is flying in a pattern consistent with a duck's migration...", the internist continues to pontificate on the various species of duck it could be, how it could be, despite all the duck-like qualities, a goose after all, and the various methods to discern what type of waterfowl one could encounter. When it comes time to shoot, the duck has flown away...
Shortly thereafter the "Quack ! Quack!" is heard again. The surgeon jumps up without hesitation and BANG!! shoots at the noise. The surgeon points to the pathologist and says, "Go tell me what that was!"
I didn't say it was a funny joke... |
MORE ON MEDICAL PATERNALISM....
In his first post in the Paternalism in Medicine series Trent Mcbride kicked off a lively debate about how the classification of certain medications as "prescription only" was driving up the cost of medicines and medical care. Well, according to this recent entry on Reason Online the same argument may be applied to medical imaging tests:
The objections to body scans are multiple. They can generate "false negatives" which may lead to further tests which can be expensive, painful, and subject to complication. While CT scans are "non-invasive" they are not completely benign. There is the risk of radiation exposure and contrast reaction. Let me quote again a portion of the above:
....usually do not provide detailed analysis or consultation about the results of the scan. The patient gets a copy of the scan results, which he can take to his own doctor if abnormalities are found....
So you go and get a body scan...and something turns up. Instead of having the test performed in the context of a patient-physician relationship, where (hopefully) some discussion of potential results has occurred you are told, "Something is abnormal, go see your doctor". When you ask for some clarification you are told that Scans-R-Us does not provide "detailed analysis or consultation about the results". Good luck and good-bye. This can, unsurprisingly, cause anxiety. Similar to the anxiety felt by women when they come in with a radiologist-performed stereotactic breast biopsy which shows cancer. The extent of her counseling was "I was told to see you and bring this (path report) with me"
There can be questions about resource allocation. Some may ask, "How many children's vaccines (or mammogram sites, or health clinics)could be funded with that money?" My answer to that is if it is your own money, spend it as you please.
Sometimes you can head something off at the pass. How many adrenal cancers have been taken care of early because of the "incidentaloma" found on a CT after an car wreck. If aortic aneurysms could be found early then they could be repaired before complications arise. A few years ago there was the story of Don Sutton and Skip Caray, broadcasters for the Atlanta Braves. Caray underwent an angioplasty because a CT scan showed a severe coronary stenosis. What prompted him to do so? Don Sutton's body scan revealed a early-stage renal cancer that was resected for cure.
In reality, Sutton and Caray are the exceptions rather than the rule. But some lives may be saved. This is a issue that shows no signs of going away.
The American College of Radiology's position is here. |
In his first post in the Paternalism in Medicine series Trent Mcbride kicked off a lively debate about how the classification of certain medications as "prescription only" was driving up the cost of medicines and medical care. Well, according to this recent entry on Reason Online the same argument may be applied to medical imaging tests:
Sometimes a little bit of information can be worse than no information at all. But is that really true when the information is about your own health? The Food and Drug Administration and the American Medical Association think it's dangerous and inconvenient for patients to look inside their own bodies on their own initiative and at their own expense.
CT (or CAT) scans and X-rays have become standard medical diagnostic tools. These non-invasive body scans are prescribed routinely by doctors to look inside a patient's body and discover what is causing symptoms from headaches to chest pains. This body scanning technology has become so well known, easily available, and inexpensive that some clinics are offering preemptive screening exams for people without any specific symptoms at alland advertising directly to the consumer.
Companies like Heart Check America and LifeScore offer patients direct access to medical scanning procedures. They do not require a doctor's prescription, and usually do not provide detailed analysis or consultation about the results of the scan. The patient gets a copy of the scan results, which he can take to his own doctor if abnormalities are found. Patients are drawn to the clinics by the possibility of stopping a life-threatening illness before symptoms are even felt, and by the peace of mind that a scan with no abnormalities can bring.
The FDA and AMA are outraged by this. They argue that CT scans have not been proven to be effective as screening teststhat normal results don't equal perfect health and abnormal results can cause a lot of worry over something that turns out not to be serious. And they worry that people will use body scans as a substitute for regular medical care.
Americans are savvy enough to know that a high-tech scan is no substitute for the personal care of a family doctor. And people willing to spend hundreds of dollars of their own money to check their health from the inside out are not likely to skimp on a visit to the doctor that is paid for by insurance. Instead, these patients are not satisfied with the passive role that traditional medical practices has scripted for them. They want to take control of their health situation, and now technology and the free market are providing that opportunity.
Pregnant women want to peek under their skin for non-medical reasons, too. In recent years, "keepsake" ultrasound photo clinics such as Fetal Fotos have sprung up in shopping centers around the nation. These clinics can take 3D pictures and videos of babies-to-be that are much more viewer-friendly than the fuzzy 2D ultrasound pictures obstetricians are specially trained to analyze.
Prenatal ultrasound has been around for decades, and is safely used to check a baby's gender and spot possible birth defects. Better pictures mean higher exposure to ultrasound for a longer time than routine medical checkups, but even the FDA admits that there is no evidence that ultrasound can physically harm a fetus. Nonetheless, the medical nannies at FDA caution against the use of ultrasound for "medically unnecessary" purposes.
Once a medical device is approved, the FDA cannot regulate how doctors use the device, so access to body scans and prenatal ultrasound is not likely to be restricted outright. Yet the battle for consumer control of medical choices is raging on many grounds, from high-tech scans to contact lenses to contraception. With so much information readily available about the benefits and risks of medical procedures and devices, consumers are increasingly likely to have their own opinions about what is best for them. Doctors, and the government, need to adjust to that new reality.
The objections to body scans are multiple. They can generate "false negatives" which may lead to further tests which can be expensive, painful, and subject to complication. While CT scans are "non-invasive" they are not completely benign. There is the risk of radiation exposure and contrast reaction. Let me quote again a portion of the above:
....usually do not provide detailed analysis or consultation about the results of the scan. The patient gets a copy of the scan results, which he can take to his own doctor if abnormalities are found....
So you go and get a body scan...and something turns up. Instead of having the test performed in the context of a patient-physician relationship, where (hopefully) some discussion of potential results has occurred you are told, "Something is abnormal, go see your doctor". When you ask for some clarification you are told that Scans-R-Us does not provide "detailed analysis or consultation about the results". Good luck and good-bye. This can, unsurprisingly, cause anxiety. Similar to the anxiety felt by women when they come in with a radiologist-performed stereotactic breast biopsy which shows cancer. The extent of her counseling was "I was told to see you and bring this (path report) with me"
There can be questions about resource allocation. Some may ask, "How many children's vaccines (or mammogram sites, or health clinics)could be funded with that money?" My answer to that is if it is your own money, spend it as you please.
Sometimes you can head something off at the pass. How many adrenal cancers have been taken care of early because of the "incidentaloma" found on a CT after an car wreck. If aortic aneurysms could be found early then they could be repaired before complications arise. A few years ago there was the story of Don Sutton and Skip Caray, broadcasters for the Atlanta Braves. Caray underwent an angioplasty because a CT scan showed a severe coronary stenosis. What prompted him to do so? Don Sutton's body scan revealed a early-stage renal cancer that was resected for cure.
In reality, Sutton and Caray are the exceptions rather than the rule. But some lives may be saved. This is a issue that shows no signs of going away.
The American College of Radiology's position is here. |
DCIS.....
A Debate on How to Treat Precancerous Breast Disease from the New York Times
The first time Jane Leffingwell was told that she had a precancerous lesion of the breast, she received the least aggressive treatment available: breast-conserving surgery, or lumpectomy.
She was 46, and her lesion, called ductal carcinoma in situ, or D.C.I.S., was deemed low grade, with a low likelihood of recurring.
But two years later, in 2001, a follow-up mammogram revealed that the lesion had returned. This time, her surgeon recommended a mastectomy, even though the recurrence did not increase her extremely low risk of dying of breast cancer.
"A mastectomy was obviously something I needed to think about," said Ms. Leffingwell, of Greenland, N.H.
The diagnosis of ductal carcinoma in situ, a noninvasive lesion of the lining of the milk ducts, has increased markedly in recent years, as a result of the widespread use of mammography. In 1983, the condition was diagnosed in 4,800 women. Two decades later, that number has soared to more than 50,000, with the vast majority of the lesions detected as microcalcifications on mammograms. D.C.I.S. is too small to be detected as a lump by a woman or her doctor.
But there is a mounting debate among experts over how aggressively to treat the disease, which has a 10-year mortality rate hovering around 1 percent. Studies, including a recent review published in The Journal of the National Cancer Institute, indicate that treatment varies widely across the country and that the form of treatment a woman receives appears to make little or no difference in survival rates.
D.C.I.S. has traditionally been treated aggressively, with mastectomy and lymph node biopsies to test for spread of the disease. But many experts now recommend the less-aggressive lumpectomy plus radiation, and some argue that women with low-grade D.C.I.S., who make up as much as 25 percent of cases, do not need radiation at all.
My partner, who does breast surgery only under extreme duress, points out the illogical treatment of breast disease by stating, "For invasive cancer you conserve the breast but for pre-invasive disease you remove it?" Much of this has to do with the potential for DCIS to return, and uncertainties concerning the biologic behavior of the disease. Treatment does seem to be moving to a more breast-conservation oriented approach:
The National Cancer Institute review, by Dr. Nancy N. Baxter, an assistant professor of surgery at the University of Minnesota in Minneapolis, found a trend in 1999 toward less aggressive therapy. For example, mastectomy was performed in 28 percent of cases, compared with 43 percent in 1992; lymph node biopsies dropped to 15 percent from 34 percent in the same period.
At the same time, the use of radiation therapy after lumpectomy has increased, rising to 54 percent in 1999 from 45 percent in 1992.
So the question remains, what to do? DCIS can be low-grade or very aggressive. Surgical margins are very important in determining need for mastectomy or radiation. As expected recurrence rates vary with treatment modality:
With lumpectomy alone, the risk of recurrence of D.C.I.S. is 30 percent over 10 years, studies have shown. Half of the recurrences are invasive breast cancer, the other half recur in the same precancerous form. Radiation, according to three large randomized clinical trials, reduces the 10-year risk of invasive breast cancer by half, to about 7 percent. Giving tamoxifen, a hormonal treatment, after radiation drops the risk to 3.5 percent. With mastectomy, the 10-year recurrence rate is 1 percent.
In a study published last year in The American Journal of Surgery, Dr. Silverstein followed women with D.C.I.S. who had characteristics suggesting they were at low risk for recurrence. Their tumors were small, they had wide margins (the space between the outermost precancerous cells and the edge of the specimen that was surgically removed), and they were of a low-grade, non-comedo type. The patients were older, so there was less time for recurrence.
After 10 years, Dr. Silverstein found the patients in the low-risk group who had lumpectomy alone had a recurrence rate of 4 percent, a rate so low that radiation would not be indicated, he said.
This study relied on the application of the Van Nuys Prognostic Index, a score based on tumor size, margins, and histologic grade. The new modification now adds the age of the patient. Each factor is assigned a numeric value and they are added together. The abstract:
The original Van Nuys prognostic index (VNPI) was introduced in 1996 as an aid to the complex treatment decision-making process for patients with ductal carcinoma in situ (DCIS) of the breast. This update adds patient age to the previous predictors of local recurrence in breast preservation patients. METHODS: A prospective database consisting of 706 conservatively patients with DCIS was examined using multivariate analysis. Four independent predictors of local recurrence (tumor size, margin width, pathologic classification, and age) were used to derive a new formula for the University of Southern California (USC)/VNPI. RESULTS: In all, 706 patients with pure DCIS were treated with breast preservation. There was no statistical difference in the 12-year local recurrence-free survival in patients with USC/VNPI scores of 4, 5, or 6, regardless of whether or not radiation therapy was used (P = not significant). Patients with USC/VNPI scores of 7, 8, or 9 received a statistically significant average 12% to 15% local recurrence-free survival benefit when treated with radiation therapy (P = 0.03). Patients with scores of 10, 11, or 12, although showing the greatest absolute benefit from radiation therapy, experienced local recurrence rates of almost 50% at 5 years. CONCLUSIONS: Ductal carcinoma in situ patients with USC/VNPI scores of 4, 5 or 6 can be considered for treatment with excision only. Patients with intermediate scores (7, 8, or 9) should be considered for treatment with radiation therapy or be reexcised if margin width is less than 10 mm and cosmetically feasible. Patients with USC/VNPI scores of 10, 11, or 12 exhibit extremely high local recurrence rates, regardless of irradiation, and should be considered for mastectomy, generally with immediate reconstruction or reexcision if technically possible.
A randomized trial is currently underway to examine if radiation can be eliminated from the treatment regimen. |
A Debate on How to Treat Precancerous Breast Disease from the New York Times
The first time Jane Leffingwell was told that she had a precancerous lesion of the breast, she received the least aggressive treatment available: breast-conserving surgery, or lumpectomy.
She was 46, and her lesion, called ductal carcinoma in situ, or D.C.I.S., was deemed low grade, with a low likelihood of recurring.
But two years later, in 2001, a follow-up mammogram revealed that the lesion had returned. This time, her surgeon recommended a mastectomy, even though the recurrence did not increase her extremely low risk of dying of breast cancer.
"A mastectomy was obviously something I needed to think about," said Ms. Leffingwell, of Greenland, N.H.
The diagnosis of ductal carcinoma in situ, a noninvasive lesion of the lining of the milk ducts, has increased markedly in recent years, as a result of the widespread use of mammography. In 1983, the condition was diagnosed in 4,800 women. Two decades later, that number has soared to more than 50,000, with the vast majority of the lesions detected as microcalcifications on mammograms. D.C.I.S. is too small to be detected as a lump by a woman or her doctor.
But there is a mounting debate among experts over how aggressively to treat the disease, which has a 10-year mortality rate hovering around 1 percent. Studies, including a recent review published in The Journal of the National Cancer Institute, indicate that treatment varies widely across the country and that the form of treatment a woman receives appears to make little or no difference in survival rates.
D.C.I.S. has traditionally been treated aggressively, with mastectomy and lymph node biopsies to test for spread of the disease. But many experts now recommend the less-aggressive lumpectomy plus radiation, and some argue that women with low-grade D.C.I.S., who make up as much as 25 percent of cases, do not need radiation at all.
My partner, who does breast surgery only under extreme duress, points out the illogical treatment of breast disease by stating, "For invasive cancer you conserve the breast but for pre-invasive disease you remove it?" Much of this has to do with the potential for DCIS to return, and uncertainties concerning the biologic behavior of the disease. Treatment does seem to be moving to a more breast-conservation oriented approach:
The National Cancer Institute review, by Dr. Nancy N. Baxter, an assistant professor of surgery at the University of Minnesota in Minneapolis, found a trend in 1999 toward less aggressive therapy. For example, mastectomy was performed in 28 percent of cases, compared with 43 percent in 1992; lymph node biopsies dropped to 15 percent from 34 percent in the same period.
At the same time, the use of radiation therapy after lumpectomy has increased, rising to 54 percent in 1999 from 45 percent in 1992.
So the question remains, what to do? DCIS can be low-grade or very aggressive. Surgical margins are very important in determining need for mastectomy or radiation. As expected recurrence rates vary with treatment modality:
With lumpectomy alone, the risk of recurrence of D.C.I.S. is 30 percent over 10 years, studies have shown. Half of the recurrences are invasive breast cancer, the other half recur in the same precancerous form. Radiation, according to three large randomized clinical trials, reduces the 10-year risk of invasive breast cancer by half, to about 7 percent. Giving tamoxifen, a hormonal treatment, after radiation drops the risk to 3.5 percent. With mastectomy, the 10-year recurrence rate is 1 percent.
In a study published last year in The American Journal of Surgery, Dr. Silverstein followed women with D.C.I.S. who had characteristics suggesting they were at low risk for recurrence. Their tumors were small, they had wide margins (the space between the outermost precancerous cells and the edge of the specimen that was surgically removed), and they were of a low-grade, non-comedo type. The patients were older, so there was less time for recurrence.
After 10 years, Dr. Silverstein found the patients in the low-risk group who had lumpectomy alone had a recurrence rate of 4 percent, a rate so low that radiation would not be indicated, he said.
This study relied on the application of the Van Nuys Prognostic Index, a score based on tumor size, margins, and histologic grade. The new modification now adds the age of the patient. Each factor is assigned a numeric value and they are added together. The abstract:
The original Van Nuys prognostic index (VNPI) was introduced in 1996 as an aid to the complex treatment decision-making process for patients with ductal carcinoma in situ (DCIS) of the breast. This update adds patient age to the previous predictors of local recurrence in breast preservation patients. METHODS: A prospective database consisting of 706 conservatively patients with DCIS was examined using multivariate analysis. Four independent predictors of local recurrence (tumor size, margin width, pathologic classification, and age) were used to derive a new formula for the University of Southern California (USC)/VNPI. RESULTS: In all, 706 patients with pure DCIS were treated with breast preservation. There was no statistical difference in the 12-year local recurrence-free survival in patients with USC/VNPI scores of 4, 5, or 6, regardless of whether or not radiation therapy was used (P = not significant). Patients with USC/VNPI scores of 7, 8, or 9 received a statistically significant average 12% to 15% local recurrence-free survival benefit when treated with radiation therapy (P = 0.03). Patients with scores of 10, 11, or 12, although showing the greatest absolute benefit from radiation therapy, experienced local recurrence rates of almost 50% at 5 years. CONCLUSIONS: Ductal carcinoma in situ patients with USC/VNPI scores of 4, 5 or 6 can be considered for treatment with excision only. Patients with intermediate scores (7, 8, or 9) should be considered for treatment with radiation therapy or be reexcised if margin width is less than 10 mm and cosmetically feasible. Patients with USC/VNPI scores of 10, 11, or 12 exhibit extremely high local recurrence rates, regardless of irradiation, and should be considered for mastectomy, generally with immediate reconstruction or reexcision if technically possible.
A randomized trial is currently underway to examine if radiation can be eliminated from the treatment regimen. |
Tuesday, June 22, 2004
MEDICAL LEADERSHIP....
Over the weekend I had the pleasure of attending the VHA Georgia Physicians Leadership College. Physician medical staff leaders from several hospitals across the state attended. The presentations were mainly concerned with how to run meetings and other such things. A recurrent theme was the need to, for lack of a better term, "spin" your message to most effectively reach your target audience. This was assisted by a tool called the "Medical Staff Menangerie". This assigned various members of the medical staff to animals based on their attitude, age, specialty, and personality type. So the lesson is that you have to approach the "young wolf" differently than the "lion king".
Based on the discussion there are a two big problems facing medical staffs in this day and age; call coverage and reimbursement and problem physicians.
The call reimbursement issue is causing a great deal of consternation where it is currently undergoing discussion. There is debate not only between physicians and hospitals but amongst physicians themselves whether call pay is a good thing or not. The hospitals are in a position of not really wanting to find additional money for call pay, but feeling pressure to do so rather than face a massive medical staff exit or revolt. Some physicians (usually older ones) regard unassigned call as a social obligation and a price to pay for hospital "privileges". They are four-square against any movement to secure additional funds. There are also issues of fairness in such a system. Does it apply only to trauma? If so, who gets the money? The general surgeons? orthopedists? plastic surgeons? Given that this question has been settled between the hospital and the Acme Surgical Corp., I am very happy. (We do get paid for call, BTW). The "pay for call" group makes their case by arguing that the requirements to take emergency call put them at risk from multiple angles. There can be a significant economic cost if you have to bump an insured patient to provide care in an emergency situation. There is a risk of litigation involved as well as outcomes under these situations may not be ideal. This combined with a general reduction of reimbursement from other sources makes such situations less attractive all the time. Remember that the ones raising these points during the meeting were not "troublemakers", but physicians who worked closely enough with hospital administrations that they were willing to foot the bill for the conference. A wise physician once told me that EMTALA turned care for the uninsured from a obligation that was freely and (to a point) gladly taken, to one that was legally mandated and now resented.
The problem physician is no longer the surgeon who throws instruments in the operating room. The physician who berates the staff and yells at them also falls into this category. Nurses nowadays are not going to tolerate the B.S. that was considered acceptable behavior in years past. The point was made that the real problem was not the incompetent physician who pitched a fit, since they were either ignored or on their way of the staff anyway. The problem is the otherwise "good" doctor who pulls these sort of stunts. This has the potential to become a patient safety issue since if a nurse gets yelled at enough for calling a physician, they won't call anymore and the patient may suffer. As medical staffs become less tolerant of such things, the policing of our ranks will improve. |
Over the weekend I had the pleasure of attending the VHA Georgia Physicians Leadership College. Physician medical staff leaders from several hospitals across the state attended. The presentations were mainly concerned with how to run meetings and other such things. A recurrent theme was the need to, for lack of a better term, "spin" your message to most effectively reach your target audience. This was assisted by a tool called the "Medical Staff Menangerie". This assigned various members of the medical staff to animals based on their attitude, age, specialty, and personality type. So the lesson is that you have to approach the "young wolf" differently than the "lion king".
Based on the discussion there are a two big problems facing medical staffs in this day and age; call coverage and reimbursement and problem physicians.
The call reimbursement issue is causing a great deal of consternation where it is currently undergoing discussion. There is debate not only between physicians and hospitals but amongst physicians themselves whether call pay is a good thing or not. The hospitals are in a position of not really wanting to find additional money for call pay, but feeling pressure to do so rather than face a massive medical staff exit or revolt. Some physicians (usually older ones) regard unassigned call as a social obligation and a price to pay for hospital "privileges". They are four-square against any movement to secure additional funds. There are also issues of fairness in such a system. Does it apply only to trauma? If so, who gets the money? The general surgeons? orthopedists? plastic surgeons? Given that this question has been settled between the hospital and the Acme Surgical Corp., I am very happy. (We do get paid for call, BTW). The "pay for call" group makes their case by arguing that the requirements to take emergency call put them at risk from multiple angles. There can be a significant economic cost if you have to bump an insured patient to provide care in an emergency situation. There is a risk of litigation involved as well as outcomes under these situations may not be ideal. This combined with a general reduction of reimbursement from other sources makes such situations less attractive all the time. Remember that the ones raising these points during the meeting were not "troublemakers", but physicians who worked closely enough with hospital administrations that they were willing to foot the bill for the conference. A wise physician once told me that EMTALA turned care for the uninsured from a obligation that was freely and (to a point) gladly taken, to one that was legally mandated and now resented.
The problem physician is no longer the surgeon who throws instruments in the operating room. The physician who berates the staff and yells at them also falls into this category. Nurses nowadays are not going to tolerate the B.S. that was considered acceptable behavior in years past. The point was made that the real problem was not the incompetent physician who pitched a fit, since they were either ignored or on their way of the staff anyway. The problem is the otherwise "good" doctor who pulls these sort of stunts. This has the potential to become a patient safety issue since if a nurse gets yelled at enough for calling a physician, they won't call anymore and the patient may suffer. As medical staffs become less tolerant of such things, the policing of our ranks will improve. |
Wednesday, June 16, 2004
BUCKLE UP...
This is something I have wanted to rant about for awhile but just haven't had the time to do so. With the coming of summer there has been an emphasis on speeding and compliance with the seat belt law in Georgia. The "Click it or Ticket" campaign finished last week. While I consider myself a libertarian in many ways (for drug legalization, against government regulation of fast food, ect), there are some ways I diverge from libertarian orthodoxy. In other words when it comes to seat belt use requirements and motorcycle helmet laws I am a "small -l" libertarian, rather than a "large L" one. Some may think me hypocritical since I resent government interference with what people put in their mouths, how they educate their children, or do in their bedrooms; but am more than willing to go along with restrictions on how one rides a motorcycle or drives a car. They may be right. I'm sure it has to do with the patients I see in my trauma practice, and how many injuries and deaths could be avoided if people would buckle up or wear helmets. Now I've heard all the anecdotal stories about car crashes where the patients say that they would not have survived the collision had they been restrained. I'm sure that such things happen, but statistically in a crash you are safer in a car which has been designed with your safety in mind than flying out into the cold, cruel world.
What got me thinking about this was an article in Reason Online last month about this topic:
Who's the bigger threat to your safety, a murderer or someone who attempts suicide? The answer is obvious, and we'd certainly jeer any mayor who suggested lowering a city's death toll by cracking down on suicides. Yet something strange happens when death comes to the highway. Politicians lock arms with law enforcement, and come up with campaigns like "Click It or Ticket," which began Monday and aims to reduce highway fatalities through stricter seat belt law enforcement. Suddenly, the murder-suicide distinction vanishes, and it's perfectly acceptable to reduce deaths by punishing those who put only themselves at risk.
But given the recent problem of interstate bridge jumpers in Atlanta, not even those who wish to take their own lives operate in a vacuum.
Further:
But if an adult does something risky-like tightrope walking, smoking or driving without a seatbelt-that person alone is responsible for the consequences. And since drivers who don't buckle up aren't making anyone else less safe, laws that bear down on these people don't make other motorists any safer either. We should be allowed to ruin our own lives, but we shouldn't be allowed to ruin the lives of others. So, yes, it's tragic when someone dies because he refused to wear a seatbelt, but it's much more tragic when a reckless driver kills innocent people. Public policy should not concern itself with decreasing all highway deaths, but with decreasing the deaths of innocents.
Sounds great, but in the real world those people are not alone responsible for their consequences. They arrive at the ED and are treated the same if they were wearing a seatbelt or helmet or not. The physicians, nurses and hospital staff who take care of these patients suffer the consequences of their actions. If these people are uninsured, the hospital suffers from the consequences of their actions. If these people qualify for disability due to the collision, then everyone suffers from the consequences of their actions.
But can't the same be said for overeating or smoking? Yes, and I pay more for my life insurance because of my weight and risk underwriting may be coming to health insurance as well.
What about such programs like the one in Florida which mandates the purchase of at least $10,000 of insurance if they wish to ride a motorcycle without a helmet? Such policies are a good idea but ten thousand dollars would be inadequate to cover much of an acute hospital stay associated with a severe injury, much less the long-term care and rehab that would be required.
The argument can be made that seatbelt use can actually lead to worse driving habits:
And seat belt laws come with their own set of unintended consequences, which further complicates the principle that policy should protect the peaceful people from the dangerous. Seat belt laws may make drivers and children safer, but economists such as Christopher Garbacz suggest that greater safety can make drivers more comfortable with dangerous driving, which puts the lives of more innocentsÂlike pedestrians, cyclists and other passengersÂin jeopardy. Risk assessment researchers have long pondered this paradox, and some have even suggested (only half jokingly) that the best way to promote cautious driving would be to attach a twelve-inch buck knife to all steering wheels.
The same can be said of anti-lock brakes, airbags, and front and rear-end crumple zones. Are there people advocating the removal of those devices from passenger cars? Those features are also mandated by the government. Does the mere fact that seatbelt use requires active participation by the occupant of the vehicle make regulations regarding their use especially burdensome?
And what of consequences? In Georgia the only consequences seem to be fines and points on your license if stopped. Other than the injuries suffered by the unrestrained occupants in a crash, there is really no downside according to Georgia law:
Ga. L. 2000, pg. 764, Code 40-8-76.1, item D
The failure of an occupant of a motor vehicle to wear a seat safety belt in any seat of a motor vehicle which has a seat safety belt or belts shall not be considered evidence of negligence or causation, shall not otherwise be considered by the finder of fact on any question of liability of any person, corporation, or insurer, shall not be any basis for cancellation of coverage or increase in insurance rates, and shall not be evidence used to diminish any recovery for damages arising out of the ownership, maintenance, occupancy, or operation of a motor vehicle.
So if you don't wear a seat belt and are injured that fact cannot be used to reduce other's liability in any lawsuits that may arise. See this case for an example of this in action. (via Overlawyered). So this adds insult to injury by nannying us into wearing our seatbelts, but removes any real consequences if we don't. You want a seatbelt law with teeth, keep the fines and points, but also codify that any injuries you sustain if not wearing a seat belt are due to your negligence and other parties cannot be held responsible for them. Even more draconian measures would allow for the waiver of EMTALA regulations under those circumstances.
In writing this I continue to struggle with the difficulty, possibly delusional, in reconciling my libertarianism with my obligations as a physician. If we were to refuse to treat those patients whose conditions were brought on by self-abuse then our waiting rooms would be empty indeed.
|
This is something I have wanted to rant about for awhile but just haven't had the time to do so. With the coming of summer there has been an emphasis on speeding and compliance with the seat belt law in Georgia. The "Click it or Ticket" campaign finished last week. While I consider myself a libertarian in many ways (for drug legalization, against government regulation of fast food, ect), there are some ways I diverge from libertarian orthodoxy. In other words when it comes to seat belt use requirements and motorcycle helmet laws I am a "small -l" libertarian, rather than a "large L" one. Some may think me hypocritical since I resent government interference with what people put in their mouths, how they educate their children, or do in their bedrooms; but am more than willing to go along with restrictions on how one rides a motorcycle or drives a car. They may be right. I'm sure it has to do with the patients I see in my trauma practice, and how many injuries and deaths could be avoided if people would buckle up or wear helmets. Now I've heard all the anecdotal stories about car crashes where the patients say that they would not have survived the collision had they been restrained. I'm sure that such things happen, but statistically in a crash you are safer in a car which has been designed with your safety in mind than flying out into the cold, cruel world.
What got me thinking about this was an article in Reason Online last month about this topic:
Who's the bigger threat to your safety, a murderer or someone who attempts suicide? The answer is obvious, and we'd certainly jeer any mayor who suggested lowering a city's death toll by cracking down on suicides. Yet something strange happens when death comes to the highway. Politicians lock arms with law enforcement, and come up with campaigns like "Click It or Ticket," which began Monday and aims to reduce highway fatalities through stricter seat belt law enforcement. Suddenly, the murder-suicide distinction vanishes, and it's perfectly acceptable to reduce deaths by punishing those who put only themselves at risk.
But given the recent problem of interstate bridge jumpers in Atlanta, not even those who wish to take their own lives operate in a vacuum.
Further:
But if an adult does something risky-like tightrope walking, smoking or driving without a seatbelt-that person alone is responsible for the consequences. And since drivers who don't buckle up aren't making anyone else less safe, laws that bear down on these people don't make other motorists any safer either. We should be allowed to ruin our own lives, but we shouldn't be allowed to ruin the lives of others. So, yes, it's tragic when someone dies because he refused to wear a seatbelt, but it's much more tragic when a reckless driver kills innocent people. Public policy should not concern itself with decreasing all highway deaths, but with decreasing the deaths of innocents.
Sounds great, but in the real world those people are not alone responsible for their consequences. They arrive at the ED and are treated the same if they were wearing a seatbelt or helmet or not. The physicians, nurses and hospital staff who take care of these patients suffer the consequences of their actions. If these people are uninsured, the hospital suffers from the consequences of their actions. If these people qualify for disability due to the collision, then everyone suffers from the consequences of their actions.
But can't the same be said for overeating or smoking? Yes, and I pay more for my life insurance because of my weight and risk underwriting may be coming to health insurance as well.
What about such programs like the one in Florida which mandates the purchase of at least $10,000 of insurance if they wish to ride a motorcycle without a helmet? Such policies are a good idea but ten thousand dollars would be inadequate to cover much of an acute hospital stay associated with a severe injury, much less the long-term care and rehab that would be required.
The argument can be made that seatbelt use can actually lead to worse driving habits:
And seat belt laws come with their own set of unintended consequences, which further complicates the principle that policy should protect the peaceful people from the dangerous. Seat belt laws may make drivers and children safer, but economists such as Christopher Garbacz suggest that greater safety can make drivers more comfortable with dangerous driving, which puts the lives of more innocentsÂlike pedestrians, cyclists and other passengersÂin jeopardy. Risk assessment researchers have long pondered this paradox, and some have even suggested (only half jokingly) that the best way to promote cautious driving would be to attach a twelve-inch buck knife to all steering wheels.
The same can be said of anti-lock brakes, airbags, and front and rear-end crumple zones. Are there people advocating the removal of those devices from passenger cars? Those features are also mandated by the government. Does the mere fact that seatbelt use requires active participation by the occupant of the vehicle make regulations regarding their use especially burdensome?
And what of consequences? In Georgia the only consequences seem to be fines and points on your license if stopped. Other than the injuries suffered by the unrestrained occupants in a crash, there is really no downside according to Georgia law:
Ga. L. 2000, pg. 764, Code 40-8-76.1, item D
The failure of an occupant of a motor vehicle to wear a seat safety belt in any seat of a motor vehicle which has a seat safety belt or belts shall not be considered evidence of negligence or causation, shall not otherwise be considered by the finder of fact on any question of liability of any person, corporation, or insurer, shall not be any basis for cancellation of coverage or increase in insurance rates, and shall not be evidence used to diminish any recovery for damages arising out of the ownership, maintenance, occupancy, or operation of a motor vehicle.
So if you don't wear a seat belt and are injured that fact cannot be used to reduce other's liability in any lawsuits that may arise. See this case for an example of this in action. (via Overlawyered). So this adds insult to injury by nannying us into wearing our seatbelts, but removes any real consequences if we don't. You want a seatbelt law with teeth, keep the fines and points, but also codify that any injuries you sustain if not wearing a seat belt are due to your negligence and other parties cannot be held responsible for them. Even more draconian measures would allow for the waiver of EMTALA regulations under those circumstances.
In writing this I continue to struggle with the difficulty, possibly delusional, in reconciling my libertarianism with my obligations as a physician. If we were to refuse to treat those patients whose conditions were brought on by self-abuse then our waiting rooms would be empty indeed.
|
Tuesday, June 15, 2004
PRACTICE WHAT WE PREACH....
Doctors tackle their own weight problems:AMA wants physicians to set an example for their patients
“I’m Michael and I’m obese.” Doctors laughed at the American Medical Association annual meeting when one of their own stood up Monday to admit his girth, but the subject was serious: physicians tackling the nation’s obesity epidemic by addressing their own weight problems.
Dr. Michael Fleming — the Shreveport, La., family physician who prompted the chuckles Monday — said he has decided to wear a pedometer and take 10,000 steps daily. It is the same advice doctors give patients and a message the American Academy of Family Physicians is relaying to its more than 90,000 members so they can serve as role models.......The separate informational obesity discussion, which drew an overflow crowd of more than 150 doctors, harkened to the AMA’s stand in 1968 urging doctors to quit smoking themselves and post no-smoking signs in their offices to set an example. The AMA is seeking to give obesity the same attention.
Before I started to work out and keep away from the Big Macs I carried 310 pounds on a 6'4" frame with a resultant BMI of 37. I felt uncomfortable discussing weight loss with patients because I felt like a hypocrite. I am now down to 270. I still don't discuss it much however. The main reason I did was to try to get hernia patients to lose weight.
Some think a good place to start is at the meetings themselves:
Some of the doctors ate high-calorie sweet rolls and muffins provided at the hotel. One doctor took the microphone and said more healthful food should be served at such meetings to set an example.
“We should start with ourselves” and offer food like bran muffins “instead of the hyper-cholesterol meals,” said Dr. Mary Ellen Bradshaw, a public health specialist from Arizona.
But there are a few voices crying out for some personal responsibility:
But Dr. Paul Handel of Houston told participants, “The obesity epidemic is not the fault of Krispy Kreme or McDonald’s. Unless we rekindle some sense of personal responsibility ... 20 years from now we will still be struggling to treat” the problem. |
Doctors tackle their own weight problems:AMA wants physicians to set an example for their patients
“I’m Michael and I’m obese.” Doctors laughed at the American Medical Association annual meeting when one of their own stood up Monday to admit his girth, but the subject was serious: physicians tackling the nation’s obesity epidemic by addressing their own weight problems.
Dr. Michael Fleming — the Shreveport, La., family physician who prompted the chuckles Monday — said he has decided to wear a pedometer and take 10,000 steps daily. It is the same advice doctors give patients and a message the American Academy of Family Physicians is relaying to its more than 90,000 members so they can serve as role models.......The separate informational obesity discussion, which drew an overflow crowd of more than 150 doctors, harkened to the AMA’s stand in 1968 urging doctors to quit smoking themselves and post no-smoking signs in their offices to set an example. The AMA is seeking to give obesity the same attention.
Before I started to work out and keep away from the Big Macs I carried 310 pounds on a 6'4" frame with a resultant BMI of 37. I felt uncomfortable discussing weight loss with patients because I felt like a hypocrite. I am now down to 270. I still don't discuss it much however. The main reason I did was to try to get hernia patients to lose weight.
Some think a good place to start is at the meetings themselves:
Some of the doctors ate high-calorie sweet rolls and muffins provided at the hotel. One doctor took the microphone and said more healthful food should be served at such meetings to set an example.
“We should start with ourselves” and offer food like bran muffins “instead of the hyper-cholesterol meals,” said Dr. Mary Ellen Bradshaw, a public health specialist from Arizona.
But there are a few voices crying out for some personal responsibility:
But Dr. Paul Handel of Houston told participants, “The obesity epidemic is not the fault of Krispy Kreme or McDonald’s. Unless we rekindle some sense of personal responsibility ... 20 years from now we will still be struggling to treat” the problem. |
ANOTHER SMALL TOWN HOSPITAL CLOSES.....
From the Athens Banner-Herald: Minnie Boswell closing: Greene County left in limbo
Come the end of June, Beth Watkins will be out of a job. But she's not so concerned about herself. The perinatal unit manager at Minnie G. Boswell Memorial Hospital knows that another hospital position won't be too hard to find. She's more worried about the patients she's been serving at the small, non-profit Greensboro hospital for the last two years - many of them uninsured and poor.
Minnie Boswell, as it's known familiarly in Greene County, will close its doors within a month, ending 55 years of service after Greene County leaders say they have exhausted efforts to maintain the funding necessary to keep the 15-bed hospital and 29-bed nursing home open.
With continuing budget problems forcing the hospital to close, local residents needing medical care will now face a long drive to a large medical facility like Athens Regional Medical Center or smaller hospitals like Putnam General in Eatonton or Morgan Memorial in Madison.
And while Greene County officials say they've done all they can - shelling out $6 million in subsidies over the past five years, including $700,000 earlier this month - some people associated with the hospital say the county hasn't done enough and passed up a viable chance to save Minnie Boswell in May.
Poor management and a difficult payer mix led to the current situation:
A heavy load of indigent patients and poor internal management have both contributed to the hospital's woes. Currently, 60 percent to 65 percent of the patients showing up at Minnie Boswell are indigent or utilize Medicaid or Medicare services, one of the reasons the hospital's struggled so much financially, said Phil Carpenter, the hospital's interim administrator.
Greene County is home to Lake Oconee and such resorts as Port Armor, Harbor Club and Reynolds Plantation. There has been a massive influx of money into the community, but it hasn't rubbed off on to the hospital:
Authority member Tom Mayers said he's confident that if and when Minnie Boswell finally does close, an entirely new hospital will open in the area within five years.
Lombard said any new hospital should be located at the Greensboro interchange on Interstate 20, where Georgia Highway 44 intersects the east-west freeway.
But Watkins worried that a for-profit hospital located near new upscale communities on Lake Oconee - what some fear will move into the vacuum created by Boswell's closing - won't help the county's poorer citizens.
According to census data, 70 percent of Greene County residents already travel outside the county for medical care - but those are the people with money, according to interim administrator Carpenter.
It seems that Minnie Boswell has fallen victim to the plight of many smaller hospitals. Frequently specialists don't want to practice in smaller towns so patients who require care from cardiologists or orthopedic surgeons, for example, travel to the larger facilities. This feeds the perception of the local hospital as "inadequate".The lack of such specialists means the income that could be realized from cath labs or operating rooms is not available to provide for improvements of the hospital. The hospital can't improve so the perception of it as a dangerous place worsens, and fewer people utilize it, and so goes the vicious cycle. You are then left with the situation that patients that can go somewhere else, do so and take their insurance with them.
I agree with the assumption that a new hospital will be built. The main reason that one has not been built so far was the inability to get a new certificate of need from the state. With the hospital closing one may be easier to come by.
|
From the Athens Banner-Herald: Minnie Boswell closing: Greene County left in limbo
Come the end of June, Beth Watkins will be out of a job. But she's not so concerned about herself. The perinatal unit manager at Minnie G. Boswell Memorial Hospital knows that another hospital position won't be too hard to find. She's more worried about the patients she's been serving at the small, non-profit Greensboro hospital for the last two years - many of them uninsured and poor.
Minnie Boswell, as it's known familiarly in Greene County, will close its doors within a month, ending 55 years of service after Greene County leaders say they have exhausted efforts to maintain the funding necessary to keep the 15-bed hospital and 29-bed nursing home open.
With continuing budget problems forcing the hospital to close, local residents needing medical care will now face a long drive to a large medical facility like Athens Regional Medical Center or smaller hospitals like Putnam General in Eatonton or Morgan Memorial in Madison.
And while Greene County officials say they've done all they can - shelling out $6 million in subsidies over the past five years, including $700,000 earlier this month - some people associated with the hospital say the county hasn't done enough and passed up a viable chance to save Minnie Boswell in May.
Poor management and a difficult payer mix led to the current situation:
A heavy load of indigent patients and poor internal management have both contributed to the hospital's woes. Currently, 60 percent to 65 percent of the patients showing up at Minnie Boswell are indigent or utilize Medicaid or Medicare services, one of the reasons the hospital's struggled so much financially, said Phil Carpenter, the hospital's interim administrator.
Greene County is home to Lake Oconee and such resorts as Port Armor, Harbor Club and Reynolds Plantation. There has been a massive influx of money into the community, but it hasn't rubbed off on to the hospital:
Authority member Tom Mayers said he's confident that if and when Minnie Boswell finally does close, an entirely new hospital will open in the area within five years.
Lombard said any new hospital should be located at the Greensboro interchange on Interstate 20, where Georgia Highway 44 intersects the east-west freeway.
But Watkins worried that a for-profit hospital located near new upscale communities on Lake Oconee - what some fear will move into the vacuum created by Boswell's closing - won't help the county's poorer citizens.
According to census data, 70 percent of Greene County residents already travel outside the county for medical care - but those are the people with money, according to interim administrator Carpenter.
It seems that Minnie Boswell has fallen victim to the plight of many smaller hospitals. Frequently specialists don't want to practice in smaller towns so patients who require care from cardiologists or orthopedic surgeons, for example, travel to the larger facilities. This feeds the perception of the local hospital as "inadequate".The lack of such specialists means the income that could be realized from cath labs or operating rooms is not available to provide for improvements of the hospital. The hospital can't improve so the perception of it as a dangerous place worsens, and fewer people utilize it, and so goes the vicious cycle. You are then left with the situation that patients that can go somewhere else, do so and take their insurance with them.
I agree with the assumption that a new hospital will be built. The main reason that one has not been built so far was the inability to get a new certificate of need from the state. With the hospital closing one may be easier to come by.
|
Monday, June 14, 2004
WHO NEEDS A SENIOR CRUISE WHEN YOU CAN HAVE THIS....
CUP & GOWN
Forget the convertible. A boob job is the latest must-have on your teen daughter's graduation list.
The number of 18-year-olds who underwent breast-implant surgery nearly tripled last year — from 3,872 in 2002 to 11,326 in 2003, according to the American Society for Aesthetic Plastic Surgery.
"There is a trend in which parents are giving implants as a gift, including as a graduation present," said Dr. Stephen Greenberg, who practices in Woodbury, L.I., and Manhattan
I can start a promotion of cholecystectomies and appendectomies for the all important "Grad and Dad" gift giving season. More likely to be appreciated in future years than implants. Available for all ages and genders. The women who I see with implants (usually with a abnormal mammogram or mass) almost all regret getting them when they were younger. |
CUP & GOWN
Forget the convertible. A boob job is the latest must-have on your teen daughter's graduation list.
The number of 18-year-olds who underwent breast-implant surgery nearly tripled last year — from 3,872 in 2002 to 11,326 in 2003, according to the American Society for Aesthetic Plastic Surgery.
"There is a trend in which parents are giving implants as a gift, including as a graduation present," said Dr. Stephen Greenberg, who practices in Woodbury, L.I., and Manhattan
I can start a promotion of cholecystectomies and appendectomies for the all important "Grad and Dad" gift giving season. More likely to be appreciated in future years than implants. Available for all ages and genders. The women who I see with implants (usually with a abnormal mammogram or mass) almost all regret getting them when they were younger. |
MORE ON WORK HOURS.....
From this month's Journal of the American College of Surgeons: Viewpoints from generation X: a survey of candidate and associate viewpoints on resident duty-hour regulations
Recently, the controversy over prolonged resident duty hours has gained national attention. In 2000, the Institute of Medicine report To err is human. Building a safer health system reported that medical errors result in more than 1 million patient injuries and 98,000 patient deaths each year.1 The Institute of Medicine report explored many possible contributors to medical errors. Of interest to the current debate, it stressed the need for a greater understanding of the relationship between physician workload and work hours to resultant fatigue, alertness, and sleep deprivation.
In 2001, the American Medical Student Association, the Committee of Interns and Residents, and Public Citizen petitioned the Occupational Safety and Health Administration for national resident duty-hour limitations to protect residents. They argued that prolonged resident duty hours placed residents at increased risk for motor vehicle crashes, obstetric complications, and poor mental health.2 Subsequently, Rep John Conyers Jr (D-MI), and Sen Jon Corzine (D-NJ) introduced The Patient and Physician Protection Act of 2001 (HR 3236)3 and The Patient and Physician Protection Act of 2002 (S 2614).4 The Patient and Physician Protection Acts called for federal limitation of resident duty hours to 80 hours per week. To preempt the federal government involvement in the regulation of resident duty hours, the Accreditation Council of Graduate Medical Education (ACGME) implemented duty-hour guidelines that limit resident duty hours to 80 per week, in-hospital call to no more frequent than every third night, and one full (24-hour) day free of patient care, all averaged over a 4-week period.5 The ACGME defines duty hours as all clinical and academic activities related to the residency program (ie, patient care [both inpatient and outpatient], administrative duties related to patient care, the provision for transfer of patient care, time spent in-house during call activities, and scheduled academic activities such as conferences). Duty hours do not include reading and preparation time spent away from the duty site.
There has been a great deal of controversy over resident duty hours and the ACGME implemented changes, but the literature is limited with regard to the viewpoints and attitudes of surgery house staff with respect to the implemented changes. The objective of this study was to evaluate the viewpoints and attitudes of surgical residents and staff physicians as they pertain to the national duty-hour guidelines.
So they surveyed the particpiants in the Candidate and Associate Society at the 2001 Clinical Congress. Here is how they broke down:
Sixty-nine percent agreed and 23% disagreed that resident on- call shift should be limited to no more often than every third night. Thirty-six percent agreed and 47.1% disagreed that residents should have a minimum of 10 hours off-duty time between shifts. Twenty-seven percent agreed and 64.7% disagreed that resident duty hours should be limited to 24 consecutive hours worked in one shift. Fifty percent agreed and 41.4% disagreed that the number of hours residents are allowed to work per week (7 days) should be limited. Twenty-five percent agreed and 62.1% disagreed that, in an effort to reduce duty hours, as the day progresses residents should have mandatory limited responsibilities. For example, if not on call, residents should not be sent to the operating room or given new patients after 4 . Twenty-five percent, 63.4%, and 11.0% of respondents reported that residents should be allowed to work, on average, ≤80 hours per week, 81 to 100 hours per week, and > 80 hours per week, respectively
So in a nutshell, surgery residents think that they should not be on call more than Q3,but when on call should not be required to leave the hospital post-call at a certain time. A majority believe that a 81 to 100-hour workweek is reasonable.
The discussion is fun to read:
Sociologists have previously described surgeons as individuals who, to save human life, are pragmatically oriented, take decisive action, and display value patterns and behaviors that are emblematic of the “hero” in American society.6,7 This perspective has been propagated by the presentation of surgeons in popular television programs such as Ben Casey, MASH, St Elsewhere, and ER, just to name a few. To live up to the societal and surgical cultural demands and expectations of the “hero,” surgical residents work long and grueling hours
Saddest day of my residency was when I had to turn in my tights and cape.
As Europe plans to implement a 48-hour resident workweek, the debate over the optimal resident duty hours in this country will continue.8,9 Surgical residency training is often considered the poster child of resident duty-hour abuse.10,11 As supporters of duty-hour limitations fight to liberate surgical residents from their “self-imposed servitude,” our findings suggest that surgical residents may agree with those who believe limiting duty hours to ≤ 80 hours/week will have a deleterious effect and should not have been implemented.12 It is unclear if this viewpoint is a reflection of perceived educational needs or surgical culture.
That is no misprint, gentle reader, Europe is going to a 48 hour workweek. Did the same thought process that believed that if the overall workweek was shortened then more workers would have to be hired come up with this plan? This survey does have some limits:
Our study population consisted of a predominance of senior residents, men, and those from university training programs; so we may have underestimated the overall proportion of residents who agree with duty-hour limits.
Another possible explanation for the difference in our results compared with previous work is that attendees of the ACS-CAS Forum are more likely to agree with the published official statement of the American College of Surgeons, which strongly disagrees with duty-hour limits.9,14 A large, more representative, study is required to fully understand the viewpoints of surgeons with regard to resident duty-hour limits and determine if support for duty-hour limits differs between resident and staff physicians.
The final verdict on work-hour limits is going to be years in arrival, as the impact won't be truly felt until residents trained under the restrictions graduate and begin to practice. My personal opinion is that the current system of work-hour limits creates an artificial environment that may not hold up in the real world.
See previous posts on the subject here, here, and here. |
From this month's Journal of the American College of Surgeons: Viewpoints from generation X: a survey of candidate and associate viewpoints on resident duty-hour regulations
Recently, the controversy over prolonged resident duty hours has gained national attention. In 2000, the Institute of Medicine report To err is human. Building a safer health system reported that medical errors result in more than 1 million patient injuries and 98,000 patient deaths each year.1 The Institute of Medicine report explored many possible contributors to medical errors. Of interest to the current debate, it stressed the need for a greater understanding of the relationship between physician workload and work hours to resultant fatigue, alertness, and sleep deprivation.
In 2001, the American Medical Student Association, the Committee of Interns and Residents, and Public Citizen petitioned the Occupational Safety and Health Administration for national resident duty-hour limitations to protect residents. They argued that prolonged resident duty hours placed residents at increased risk for motor vehicle crashes, obstetric complications, and poor mental health.2 Subsequently, Rep John Conyers Jr (D-MI), and Sen Jon Corzine (D-NJ) introduced The Patient and Physician Protection Act of 2001 (HR 3236)3 and The Patient and Physician Protection Act of 2002 (S 2614).4 The Patient and Physician Protection Acts called for federal limitation of resident duty hours to 80 hours per week. To preempt the federal government involvement in the regulation of resident duty hours, the Accreditation Council of Graduate Medical Education (ACGME) implemented duty-hour guidelines that limit resident duty hours to 80 per week, in-hospital call to no more frequent than every third night, and one full (24-hour) day free of patient care, all averaged over a 4-week period.5 The ACGME defines duty hours as all clinical and academic activities related to the residency program (ie, patient care [both inpatient and outpatient], administrative duties related to patient care, the provision for transfer of patient care, time spent in-house during call activities, and scheduled academic activities such as conferences). Duty hours do not include reading and preparation time spent away from the duty site.
There has been a great deal of controversy over resident duty hours and the ACGME implemented changes, but the literature is limited with regard to the viewpoints and attitudes of surgery house staff with respect to the implemented changes. The objective of this study was to evaluate the viewpoints and attitudes of surgical residents and staff physicians as they pertain to the national duty-hour guidelines.
So they surveyed the particpiants in the Candidate and Associate Society at the 2001 Clinical Congress. Here is how they broke down:
Sixty-nine percent agreed and 23% disagreed that resident on- call shift should be limited to no more often than every third night. Thirty-six percent agreed and 47.1% disagreed that residents should have a minimum of 10 hours off-duty time between shifts. Twenty-seven percent agreed and 64.7% disagreed that resident duty hours should be limited to 24 consecutive hours worked in one shift. Fifty percent agreed and 41.4% disagreed that the number of hours residents are allowed to work per week (7 days) should be limited. Twenty-five percent agreed and 62.1% disagreed that, in an effort to reduce duty hours, as the day progresses residents should have mandatory limited responsibilities. For example, if not on call, residents should not be sent to the operating room or given new patients after 4 . Twenty-five percent, 63.4%, and 11.0% of respondents reported that residents should be allowed to work, on average, ≤80 hours per week, 81 to 100 hours per week, and > 80 hours per week, respectively
So in a nutshell, surgery residents think that they should not be on call more than Q3,but when on call should not be required to leave the hospital post-call at a certain time. A majority believe that a 81 to 100-hour workweek is reasonable.
The discussion is fun to read:
Sociologists have previously described surgeons as individuals who, to save human life, are pragmatically oriented, take decisive action, and display value patterns and behaviors that are emblematic of the “hero” in American society.6,7 This perspective has been propagated by the presentation of surgeons in popular television programs such as Ben Casey, MASH, St Elsewhere, and ER, just to name a few. To live up to the societal and surgical cultural demands and expectations of the “hero,” surgical residents work long and grueling hours
Saddest day of my residency was when I had to turn in my tights and cape.
As Europe plans to implement a 48-hour resident workweek, the debate over the optimal resident duty hours in this country will continue.8,9 Surgical residency training is often considered the poster child of resident duty-hour abuse.10,11 As supporters of duty-hour limitations fight to liberate surgical residents from their “self-imposed servitude,” our findings suggest that surgical residents may agree with those who believe limiting duty hours to ≤ 80 hours/week will have a deleterious effect and should not have been implemented.12 It is unclear if this viewpoint is a reflection of perceived educational needs or surgical culture.
That is no misprint, gentle reader, Europe is going to a 48 hour workweek. Did the same thought process that believed that if the overall workweek was shortened then more workers would have to be hired come up with this plan? This survey does have some limits:
Our study population consisted of a predominance of senior residents, men, and those from university training programs; so we may have underestimated the overall proportion of residents who agree with duty-hour limits.
Another possible explanation for the difference in our results compared with previous work is that attendees of the ACS-CAS Forum are more likely to agree with the published official statement of the American College of Surgeons, which strongly disagrees with duty-hour limits.9,14 A large, more representative, study is required to fully understand the viewpoints of surgeons with regard to resident duty-hour limits and determine if support for duty-hour limits differs between resident and staff physicians.
The final verdict on work-hour limits is going to be years in arrival, as the impact won't be truly felt until residents trained under the restrictions graduate and begin to practice. My personal opinion is that the current system of work-hour limits creates an artificial environment that may not hold up in the real world.
See previous posts on the subject here, here, and here. |
Sunday, June 13, 2004
I ALREADY LIVE IN A HOME....THEN WE'LL PUT YOU IN THE CROOKED ONE WE SAW ON "60 MINUTES"....
Hundreds of patients stand to lose state aid
Sibyl Talbot of Columbus worked from the age of 17 until she was no longer able.
Now 77, she was diagnosed with Alzheimer's disease seven years ago and is confined to Muscogee Manor & Rehabilitation Center in Columbus.
"Mother is nonverbal, nonambulatory and can't eat regular food anymore," her daughter, Linda Denney, said Friday.
Yet earlier last week, Denney said the family was notified by the Medicaid program that starting July 1 her mother will no longer receive Medicaid benefits that enable her to stay in the nursing home because she makes $1,710 a month -- or $18 more than the normal cap to receive Medicaid coverage.
A year ago, Talbot was classified as "medically needy" by the Georgia Department of Community Health. A year ago she was included in a program under which the state approves Medicaid benefits for those who make more than the $1,692 cap but not enough to pay for nursing home costs, which can be $4,000 a month or more.
But on July 1 the state is eliminating the program supporting the medically needy that serves 1,680 people across Georgia. That decision was recommended last fall by the department's board, after Gov. Sonny Perdue asked for a second round of budget cuts.
Georgia Medicaid and nusing homes....the same combination that was under investigation earlier this year for the "bed tax".
Nursing homes and families of the 1,680 Georgia nursing home residents who face cutoff of Medicaid benefits are scrambling to find some way to retain those benefits. The state has offered the special Medicaid program since 1990.
Julie Kerlin, spokeswoman for Community Health, said the state will save about $9.7 million annually by eliminating the program, and that it was a very tough decision. Overall, she said, it will mean a reduction of $24 million to the department, including the loss of federal funds.
So a program that thinks nothing of paying $107 million for a consulting firm can't find $9.7 million to keep poor folks in the nursing home.
And there are people who want to put the government in charge of all healthcare? Be careful what you ask for. |
Hundreds of patients stand to lose state aid
Sibyl Talbot of Columbus worked from the age of 17 until she was no longer able.
Now 77, she was diagnosed with Alzheimer's disease seven years ago and is confined to Muscogee Manor & Rehabilitation Center in Columbus.
"Mother is nonverbal, nonambulatory and can't eat regular food anymore," her daughter, Linda Denney, said Friday.
Yet earlier last week, Denney said the family was notified by the Medicaid program that starting July 1 her mother will no longer receive Medicaid benefits that enable her to stay in the nursing home because she makes $1,710 a month -- or $18 more than the normal cap to receive Medicaid coverage.
A year ago, Talbot was classified as "medically needy" by the Georgia Department of Community Health. A year ago she was included in a program under which the state approves Medicaid benefits for those who make more than the $1,692 cap but not enough to pay for nursing home costs, which can be $4,000 a month or more.
But on July 1 the state is eliminating the program supporting the medically needy that serves 1,680 people across Georgia. That decision was recommended last fall by the department's board, after Gov. Sonny Perdue asked for a second round of budget cuts.
Georgia Medicaid and nusing homes....the same combination that was under investigation earlier this year for the "bed tax".
Nursing homes and families of the 1,680 Georgia nursing home residents who face cutoff of Medicaid benefits are scrambling to find some way to retain those benefits. The state has offered the special Medicaid program since 1990.
Julie Kerlin, spokeswoman for Community Health, said the state will save about $9.7 million annually by eliminating the program, and that it was a very tough decision. Overall, she said, it will mean a reduction of $24 million to the department, including the loss of federal funds.
So a program that thinks nothing of paying $107 million for a consulting firm can't find $9.7 million to keep poor folks in the nursing home.
And there are people who want to put the government in charge of all healthcare? Be careful what you ask for. |
Saturday, June 12, 2004
MORE ON FRONTLINE MEDICINE....
Galen's Log recently had an excellent post about the practice of medicine in Iraq. Sounds as if the equipment we take for granted is at a premium:
The plastic laryngoscopes are bad. The blades repeatedly fall off the handle while in the patient's mouth. We are trying to order a good old fashion metal set. I have a set that I acquired from a previous deployment. I won't be leaving that behind. Also, the plastic sets have only one 4MAC and one 4Miller, no peds sizes.
Angiocaths are another hot item, not those "ProtectIVs" that we use in the hospital. We use those to start subclavian lines, then use a RIC Kit to convert it to a 7FR line. We have acquired/borrowed some.....
Individuals who do not know how to effectively use ultrasound are going to lack a diagnostic tool. John and I have ultrasounded over 100 casualties in less than 3 months. The surgeons with us depend on us to do it.
Xray is very limited. Chest tubes are put in based on clinic exam, not xray. What is a post-intubation xray? Xray after subclavian line placement? Practice patterns change based on the environment. I do not feel we are practicing bad medicine, on the contrary, I am practicing better clinic medicine than I probably ever have. As I told one Internist out here, at Camp Pendleton you can order whatever you want, here you can maybe get a simple CBC and drip your own urines. Then you have to make a decision.
Another take on medical adventures in Iraq can be found in the March 2004 Bulletin of the American College of Surgeons which tells the story of the Forward Surgical Team:
We were actually the first forward surgical team to parachute into combat since World War II......The need for a small, easy-to-insert surgical capability became evident during the U.S.-led invasion of Grenada in 1983. At that time, the smallest Army unit that could perform surgery was a mobile Army surgical hospital (MASH). Because of its large weight and size, the first MASH did not make it into Grenada until four days after the invasion started. This prompted the Army to develop the FST to meet the need for a small, readily deployed surgical team that could perform resuscitative trauma surgical procedures on U.S. soldiers from the moment the fighting began. By 1986, Army surgical squads were organized and actually jumped in with U.S. paratroops during the invasion of Panama in 1989. These small squads had to wait for aircraft to land before they could access their operating tables, anesthesia machines, and other heavy equipment. The U.S. Army fielded the first airborne FSTs in the early 1990s. These units had the advantage of being able to parachute their heavy operating room tents, generators, and equipment into the combat zone ahead of the paratroopers on parachute-rigged Humvees. This system ensured that wounded GIs would have immediate access to lifesaving trauma resuscitation within the Âgolden hour from the moment the fighting started. The FST also enabled U.S. casualties to survive long-distance air transport back to larger hospitals located in Germany and in the continental U.S. Each FST in Operation Iraqi Freedom consisted of 20 personnel: four surgeons, five nurses, a medical operations officer, and 10 enlisted medics who specialize not only in trauma surgical procedures but also in the pre- and postoperative care of combat casualties. All surgeons and nurses were board-certified in their respective specialties and used state-of-the-art equipment and techniques to provide the best trauma care to U.S. troops who happened to be injured in the line of duty. "By far, the most useful item was the Sonosite portable ultrasound," says Dr. Rush. "The FAST exam was very useful as a triage tool, as the injured paratroopers we work on have tremendous physiologic reserve. This diminishes the reliability of routine vital signs in making triage decisions. We also used the Sonosite to screen for traumatic pseudoaneurysms, assess the adequacy of vascular repairs, and eventually even assess congenital heart defects in young Iraqi children."
A friend of mine who finished a few years behind me is currently serving as a navy surgeon in a far outpost of the realm. They have no neurosurgeons or thoracic surgeons. The personel there told him to do as many thoractomies and craniotomies as he could so he would be prepared. He has done about four of each in trauma patients since he has been there. He likes it, but probably not enough to re-enlist. |
Galen's Log recently had an excellent post about the practice of medicine in Iraq. Sounds as if the equipment we take for granted is at a premium:
The plastic laryngoscopes are bad. The blades repeatedly fall off the handle while in the patient's mouth. We are trying to order a good old fashion metal set. I have a set that I acquired from a previous deployment. I won't be leaving that behind. Also, the plastic sets have only one 4MAC and one 4Miller, no peds sizes.
Angiocaths are another hot item, not those "ProtectIVs" that we use in the hospital. We use those to start subclavian lines, then use a RIC Kit to convert it to a 7FR line. We have acquired/borrowed some.....
Individuals who do not know how to effectively use ultrasound are going to lack a diagnostic tool. John and I have ultrasounded over 100 casualties in less than 3 months. The surgeons with us depend on us to do it.
Xray is very limited. Chest tubes are put in based on clinic exam, not xray. What is a post-intubation xray? Xray after subclavian line placement? Practice patterns change based on the environment. I do not feel we are practicing bad medicine, on the contrary, I am practicing better clinic medicine than I probably ever have. As I told one Internist out here, at Camp Pendleton you can order whatever you want, here you can maybe get a simple CBC and drip your own urines. Then you have to make a decision.
Another take on medical adventures in Iraq can be found in the March 2004 Bulletin of the American College of Surgeons which tells the story of the Forward Surgical Team:
We were actually the first forward surgical team to parachute into combat since World War II......The need for a small, easy-to-insert surgical capability became evident during the U.S.-led invasion of Grenada in 1983. At that time, the smallest Army unit that could perform surgery was a mobile Army surgical hospital (MASH). Because of its large weight and size, the first MASH did not make it into Grenada until four days after the invasion started. This prompted the Army to develop the FST to meet the need for a small, readily deployed surgical team that could perform resuscitative trauma surgical procedures on U.S. soldiers from the moment the fighting began. By 1986, Army surgical squads were organized and actually jumped in with U.S. paratroops during the invasion of Panama in 1989. These small squads had to wait for aircraft to land before they could access their operating tables, anesthesia machines, and other heavy equipment. The U.S. Army fielded the first airborne FSTs in the early 1990s. These units had the advantage of being able to parachute their heavy operating room tents, generators, and equipment into the combat zone ahead of the paratroopers on parachute-rigged Humvees. This system ensured that wounded GIs would have immediate access to lifesaving trauma resuscitation within the Âgolden hour from the moment the fighting started. The FST also enabled U.S. casualties to survive long-distance air transport back to larger hospitals located in Germany and in the continental U.S. Each FST in Operation Iraqi Freedom consisted of 20 personnel: four surgeons, five nurses, a medical operations officer, and 10 enlisted medics who specialize not only in trauma surgical procedures but also in the pre- and postoperative care of combat casualties. All surgeons and nurses were board-certified in their respective specialties and used state-of-the-art equipment and techniques to provide the best trauma care to U.S. troops who happened to be injured in the line of duty. "By far, the most useful item was the Sonosite portable ultrasound," says Dr. Rush. "The FAST exam was very useful as a triage tool, as the injured paratroopers we work on have tremendous physiologic reserve. This diminishes the reliability of routine vital signs in making triage decisions. We also used the Sonosite to screen for traumatic pseudoaneurysms, assess the adequacy of vascular repairs, and eventually even assess congenital heart defects in young Iraqi children."
A friend of mine who finished a few years behind me is currently serving as a navy surgeon in a far outpost of the realm. They have no neurosurgeons or thoracic surgeons. The personel there told him to do as many thoractomies and craniotomies as he could so he would be prepared. He has done about four of each in trauma patients since he has been there. He likes it, but probably not enough to re-enlist. |
Friday, June 11, 2004
MAMMOGRAMS....
Dr. Smith has a post today on what radiologists have told me is the "most dangerous thing they do", read mammograms. Quoting from this CNN.com report the number of mammography sites has decreased 8.9 percent since 2000. Other items of interest:
The decline is thought to be due to low insurance reimbursement for mammograms, rising malpractice litigation and fewer radiologists choosing breast imaging instead of other specialties, the scientific committee said.
At the current Medicare reimbursement of about $60 per study, the risk is becoming not worth the reward.
At the same time, the number of false-positive mammogram readings -- when something suspicious turns out to be noncancerous -- has nearly doubled, the report found. That may be due partly to radiologists practicing "defensive medicine" in hopes of avoiding lawsuits.
This is more widespread than you may think. I have had several BIRADS 4 lesions that "disappear" when sent for localization just a few weeks after the initial mammograms are taken. I am also seeing many long-standing lesions that were called BIRADS 2 in previous years now called BIRADS 3. These patients are not usually biopsied right away but may have short-term (6 month) mammograms. This can be stressful in and of itself.
Some solutions offered:
Mammography facilities specially train nonphysician workers to prescreen mammograms. These employees would not replace radiologists but would do some of the less critical work so sites can perform more scans.
So on the one hand the article laments the lack of breast-fellowship trained radiologists and cites the high risk of litigation involved with mammography, while on the other hand want non-physicians to "prescreen" them. Given the malpractice climate now I think this is a non-starter.
The easy-to-perform X-ray be offered at more locations but that mammograms be read at a few centralized sites, to maximize the number of radiologists.
This could work for screening mammograms, but not for diagnostic studies which usually have a radiologist on site for a on-the-spot read.
The CodeBlueBlog, written by a radiologist, has some thoughts here. |
Dr. Smith has a post today on what radiologists have told me is the "most dangerous thing they do", read mammograms. Quoting from this CNN.com report the number of mammography sites has decreased 8.9 percent since 2000. Other items of interest:
The decline is thought to be due to low insurance reimbursement for mammograms, rising malpractice litigation and fewer radiologists choosing breast imaging instead of other specialties, the scientific committee said.
At the current Medicare reimbursement of about $60 per study, the risk is becoming not worth the reward.
At the same time, the number of false-positive mammogram readings -- when something suspicious turns out to be noncancerous -- has nearly doubled, the report found. That may be due partly to radiologists practicing "defensive medicine" in hopes of avoiding lawsuits.
This is more widespread than you may think. I have had several BIRADS 4 lesions that "disappear" when sent for localization just a few weeks after the initial mammograms are taken. I am also seeing many long-standing lesions that were called BIRADS 2 in previous years now called BIRADS 3. These patients are not usually biopsied right away but may have short-term (6 month) mammograms. This can be stressful in and of itself.
Some solutions offered:
Mammography facilities specially train nonphysician workers to prescreen mammograms. These employees would not replace radiologists but would do some of the less critical work so sites can perform more scans.
So on the one hand the article laments the lack of breast-fellowship trained radiologists and cites the high risk of litigation involved with mammography, while on the other hand want non-physicians to "prescreen" them. Given the malpractice climate now I think this is a non-starter.
The easy-to-perform X-ray be offered at more locations but that mammograms be read at a few centralized sites, to maximize the number of radiologists.
This could work for screening mammograms, but not for diagnostic studies which usually have a radiologist on site for a on-the-spot read.
The CodeBlueBlog, written by a radiologist, has some thoughts here. |
Thursday, June 10, 2004
THE VORTEX.......
Today was one of those days that just when I though I was about to get out of the hospital, I got sucked right back in. The resident/staff service can do that to you. Just a few of the poor souls who have crossed my path over the past week:
60-ish woman with several month h/o weight loss, abdominal pain, and right lower quadrant mass. Has a cecal cancer with liver mets. Her resection was actually easier than I thought it would be, given the size of the mass was 10 x 10 x 8 cm.
Late 20's with a chromosomal abnormality, chronic pancreatitis, gastroparesis, recurrent DVT/PE and a enterocutaneous fistula. The fistula is from a jejunostomy tube site which was brought out through the main incision (not through a separate incision). He is status-post a pancreatico-jejunostomy, gastric pacemaker and the above feeding jejunostomy, all done at big academic centers in a galaxy far far away. Because of insurance denials and the big centers cutting their losses, they have sort of inherited me. I've placed a caval filter and a few long-term lines in him. He was in the hospital a few months ago with a line infection. The tunneled line was removed and a temporary triple lumen was placed. Against my advice his primary care team sent him home with it, and inevitably he came back with a line infection. His mother works in the hospital and tends to dictate his care. I replaced the line and obtained a duplex which showed DVT in his right IJ and bilateral subclavian veins. Again, to my chagrin, he was sent home with the triple lumen as his access AGAIN!! He comes in my office and we schedule his long-term catheter. We find he has no suitable conduit between his left IJ and his cava. He and his family are adamant, almost to the point of being pathologic, about not having a groin line. He will probably become an "access death". He will either die from a lack of access, or die while having one placed.
Three teenagers in an auto versus tree collision. Driver with right pneumo, bilteral open femur fractures, and the worst-looking open tib-fib fracture I've seen. Front-seat passenger with intercerebreal contusion, splenic and left renal laceration, and a small bowel injury. Backseat passenger with humerus fracture.
I did finally get out to get my boys to the barbershop for long-overdue haircut. |
Today was one of those days that just when I though I was about to get out of the hospital, I got sucked right back in. The resident/staff service can do that to you. Just a few of the poor souls who have crossed my path over the past week:
60-ish woman with several month h/o weight loss, abdominal pain, and right lower quadrant mass. Has a cecal cancer with liver mets. Her resection was actually easier than I thought it would be, given the size of the mass was 10 x 10 x 8 cm.
Late 20's with a chromosomal abnormality, chronic pancreatitis, gastroparesis, recurrent DVT/PE and a enterocutaneous fistula. The fistula is from a jejunostomy tube site which was brought out through the main incision (not through a separate incision). He is status-post a pancreatico-jejunostomy, gastric pacemaker and the above feeding jejunostomy, all done at big academic centers in a galaxy far far away. Because of insurance denials and the big centers cutting their losses, they have sort of inherited me. I've placed a caval filter and a few long-term lines in him. He was in the hospital a few months ago with a line infection. The tunneled line was removed and a temporary triple lumen was placed. Against my advice his primary care team sent him home with it, and inevitably he came back with a line infection. His mother works in the hospital and tends to dictate his care. I replaced the line and obtained a duplex which showed DVT in his right IJ and bilateral subclavian veins. Again, to my chagrin, he was sent home with the triple lumen as his access AGAIN!! He comes in my office and we schedule his long-term catheter. We find he has no suitable conduit between his left IJ and his cava. He and his family are adamant, almost to the point of being pathologic, about not having a groin line. He will probably become an "access death". He will either die from a lack of access, or die while having one placed.
Three teenagers in an auto versus tree collision. Driver with right pneumo, bilteral open femur fractures, and the worst-looking open tib-fib fracture I've seen. Front-seat passenger with intercerebreal contusion, splenic and left renal laceration, and a small bowel injury. Backseat passenger with humerus fracture.
I did finally get out to get my boys to the barbershop for long-overdue haircut. |
Monday, June 07, 2004
RONALD WILSON REAGAN 1911-2004
I've meant to post this since last night, but you know, stupid day job. Dr. Smith, GruntDoc and Dr. Rangel all have excellent posts about the late president.
How does the old saying go? "Show me the newspaper headlines when someone is twenty years old and I will tell you how they think today," President Reagan's term was during the point in my life that I became interested in politics and the workings of government. His frankness, optimism, and his conservatism all shaped my thinking about such things.
My best Reagan memory was when I was in high school I went to Washington, DC with a school group participating in Close Up, an alumna from our school had a job in the White House so we got to go on a special tour of the place. Great pictures of me standing behind the podium in the briefing room. Anyway the President was flying out to something that day so we got to stand behind the ropeline on the south lawn as Reagan got aboard Marine One. Heady stuff for a high school kid. |
I've meant to post this since last night, but you know, stupid day job. Dr. Smith, GruntDoc and Dr. Rangel all have excellent posts about the late president.
How does the old saying go? "Show me the newspaper headlines when someone is twenty years old and I will tell you how they think today," President Reagan's term was during the point in my life that I became interested in politics and the workings of government. His frankness, optimism, and his conservatism all shaped my thinking about such things.
My best Reagan memory was when I was in high school I went to Washington, DC with a school group participating in Close Up, an alumna from our school had a job in the White House so we got to go on a special tour of the place. Great pictures of me standing behind the podium in the briefing room. Anyway the President was flying out to something that day so we got to stand behind the ropeline on the south lawn as Reagan got aboard Marine One. Heady stuff for a high school kid. |
Saturday, June 05, 2004
BATTLE OF THE BABY HOSPITALS....
From the Atlanta Journal-Constitution (free registration required):
Children's hospital expansion approved
Children's Healthcare of Atlanta won state approval Friday for a $344 million expansion of its Egleston and Scottish Rite campuses. But the groundbreaking still might be a long way off.
The expansion has been opposed by Grady Health System, and if it appeals, the project could be delayed for months or even years.
Grady has argued that the expansion would lead to the demise of its own children's hospital. Grady officials declined to comment Friday on whether they intend to appeal the state's decision.
The Children's Healthcare plan to expand its two hospitals, Egleston and Scottish Rite, would be the most expensive hospital construction project in state history. It would increase the number of beds at both hospitals and expand emergency room capacity and other services, including space for support services for patients' families.
Children's Healthcare says it needs to grow to serve Atlanta's rising population of children and the current heavy load of patients.
In January, when Children's Healthcare filed its applications for expansion, its chief executive officer, James Tally, said the number of children in metro Atlanta is expected to increase by 140,000 by 2007, growing faster than in any other U.S. city.
Grady CEO Andrew Agwunobi, in announcing Grady's challenge to the planned project, said in April that the Children's expansion would force the shutdown of Grady's 82-bed Hughes Spalding Children's Hospital. Some of the financial success of Children's Healthcare has come at the expense of the Grady facility, Agwunobi said.
Hospitals must have a state certificate of need for major construction or expansion projects. The state bases its decision on community health care needs, and the process includes weighing arguments from organizations opposing the project.
Children's Healthcare, through a spokesman, declined to comment on Friday's approval, given by a unit of the state Department of Community Health.
Grady has 30 days to appeal to the state. If it ends up losing that appeal, it then could pursue a lawsuit to overturn the decision in Georgia courts.
Opposition to a state license can postpone the start of a hospital construction project for two years or more. Completion of the Children's Healthcare expansion had been targeted for 2007.
It's unusual for a metro area to have three children's hospitals, said Lew Yeouze, an Atlanta-based consultant for Mercer Human Resource Consulting. "In other metro areas, you have one, maybe two,'' he said.
Grady probably sees the dispute as ''another battle in a bigger war'' to relieve financial pressure and gain access to insured patients, Yeouze added.
Children's Healthcare of Atlanta was created by the 1998 merger of Egleston Children's Health Care System and Scottish Rite Children's Medical Center, which had been longtime rivals. Since the merger, the organization has emerged as a dominant hospital player in metro Atlanta.
Michael Rovinsky, president of Atlanta-based Integrity Consulting Group, a consulting firm, said Children's Healthcare and Grady ''serve two different markets, economically and geographically.''
Children's Healthcare draws more affluent and suburban families, while Hughes Spalding serves a higher percentage of inner-city patients, Rovinsky said. The quality of care at the two organizations is similar, he said.
Rovinsky added that he expects the state's decision to be upheld.
''For the markets that Children's serves, these projects are needed,'' he said
The loss of the children's hospital could hit Grady pretty hard and require it to cut back on more services. I want to bring special attention to the second-to-last paragraph:
Children's Healthcare draws more affluent and suburban families, while Hughes Spalding serves a higher percentage of inner-city patients, Rovinsky said. The quality of care at the two organizations is similar, he said.
One of the ways that Children's Healthcare of Atlanta has managed to accomplish this is by the effective job they have done in marketing themselves as a referral center. Their phone numbers are displayed at many areas of the pediatric floor. When I call the 1-800 number I speak to a physician, not a case manager or a machine, and I get on-the-spot acceptance of the patient. To my knowledge, Grady has no comparable program. |
From the Atlanta Journal-Constitution (free registration required):
Children's hospital expansion approved
Children's Healthcare of Atlanta won state approval Friday for a $344 million expansion of its Egleston and Scottish Rite campuses. But the groundbreaking still might be a long way off.
The expansion has been opposed by Grady Health System, and if it appeals, the project could be delayed for months or even years.
Grady has argued that the expansion would lead to the demise of its own children's hospital. Grady officials declined to comment Friday on whether they intend to appeal the state's decision.
The Children's Healthcare plan to expand its two hospitals, Egleston and Scottish Rite, would be the most expensive hospital construction project in state history. It would increase the number of beds at both hospitals and expand emergency room capacity and other services, including space for support services for patients' families.
Children's Healthcare says it needs to grow to serve Atlanta's rising population of children and the current heavy load of patients.
In January, when Children's Healthcare filed its applications for expansion, its chief executive officer, James Tally, said the number of children in metro Atlanta is expected to increase by 140,000 by 2007, growing faster than in any other U.S. city.
Grady CEO Andrew Agwunobi, in announcing Grady's challenge to the planned project, said in April that the Children's expansion would force the shutdown of Grady's 82-bed Hughes Spalding Children's Hospital. Some of the financial success of Children's Healthcare has come at the expense of the Grady facility, Agwunobi said.
Hospitals must have a state certificate of need for major construction or expansion projects. The state bases its decision on community health care needs, and the process includes weighing arguments from organizations opposing the project.
Children's Healthcare, through a spokesman, declined to comment on Friday's approval, given by a unit of the state Department of Community Health.
Grady has 30 days to appeal to the state. If it ends up losing that appeal, it then could pursue a lawsuit to overturn the decision in Georgia courts.
Opposition to a state license can postpone the start of a hospital construction project for two years or more. Completion of the Children's Healthcare expansion had been targeted for 2007.
It's unusual for a metro area to have three children's hospitals, said Lew Yeouze, an Atlanta-based consultant for Mercer Human Resource Consulting. "In other metro areas, you have one, maybe two,'' he said.
Grady probably sees the dispute as ''another battle in a bigger war'' to relieve financial pressure and gain access to insured patients, Yeouze added.
Children's Healthcare of Atlanta was created by the 1998 merger of Egleston Children's Health Care System and Scottish Rite Children's Medical Center, which had been longtime rivals. Since the merger, the organization has emerged as a dominant hospital player in metro Atlanta.
Michael Rovinsky, president of Atlanta-based Integrity Consulting Group, a consulting firm, said Children's Healthcare and Grady ''serve two different markets, economically and geographically.''
Children's Healthcare draws more affluent and suburban families, while Hughes Spalding serves a higher percentage of inner-city patients, Rovinsky said. The quality of care at the two organizations is similar, he said.
Rovinsky added that he expects the state's decision to be upheld.
''For the markets that Children's serves, these projects are needed,'' he said
The loss of the children's hospital could hit Grady pretty hard and require it to cut back on more services. I want to bring special attention to the second-to-last paragraph:
Children's Healthcare draws more affluent and suburban families, while Hughes Spalding serves a higher percentage of inner-city patients, Rovinsky said. The quality of care at the two organizations is similar, he said.
One of the ways that Children's Healthcare of Atlanta has managed to accomplish this is by the effective job they have done in marketing themselves as a referral center. Their phone numbers are displayed at many areas of the pediatric floor. When I call the 1-800 number I speak to a physician, not a case manager or a machine, and I get on-the-spot acceptance of the patient. To my knowledge, Grady has no comparable program. |
OBESITY AND YOU....
Apparently one of Dr. Parker's favorite tourist spots has played host to a nanny-state conference on obesity the past few days. Radley Balko has been covering it in TechCentralStation posts here, here, and here. As well as at the Cato Institute and his own blog. From what the Surgeon-General has to say, Mr. McBride should be very afraid:
If you check out the website for the Obesity Summit, you'll notice on the homepage the quote the summit's organizers have chosen to set the tone for three day event. It's from U.S. Surgeon General Richard Carmona:
"As we look to the future and where childhood obesity will be in 20 years... it is every bit as threatening to us as is the terrorist threat we face today. It is the threat from within."
The U.S. government's spokesperson on medical issues says obesity is every bit as threatening as terrorism. Given that the war on terror has spawned the largest federal bureaucracy in the history of the country, questionable trespasses on our civil liberties, and is costing U.S. taxpayers tens of billions of dollars, that's an awfully scary thing for a high-ranking government official to say. And that conference organizers chose to place Carmona's quote front and center ought to give some sort of indication of the starting point from which this debate's about to kick off."
So I guess that means the deck is stacked already. The third TCS article is an excellent analysis of the myth that medical underwriting is illegal:
When I was originally asked to write the designated dissent piece for TIME's special issue on obesity, I went back and forth with a fact-checker over my assertion that state and federal governments prevented health insurers from tying health insurance premiums to risk -- the same way car and life insurers do. Charging everyone within a group plan the same amount for health insurance removes an important financial incentive to stay healthy, and forces fit people to subsidize health care for the not-so-fit. Allowing folks who keep the weight off and the blood pressure and cholesterol down to pay less for health insurance (and allowing health insurers to provide it to them) would also strike a needed blow for personal responsibility in the obesity debate.
The problem is that though several health care policy experts told me they were certain health insurers were barred from such "medical underwriting," no one could say exactly why. In fact, I talked to several health insurance companies themselves, and none could point to any specific law, regulation, or case law laying out the prohibition. I even called tort king John Banzhaf, who -- believe it or not -- is actually on record supporting lower premiums for fit health care consumes, though only as it applies to obesity and blood pressure.....I called the general counsel's office at HHS. Deputy General Counsel Paula Stannard walked me through every possible federal barrier to medical underwriting, and explained why they don't apply.
In fact, in 2001 the Depts. of HHS, Labor and the Treasury (in predictable federal bureaucratic confusion, the three agencies share jurisdiction over the issue) proposed a regulation (66 Fed. Reg. 1421) insisting that the convoluted HIPAA (Health Insurance Portability and Accountability Act) regulations be interpreted to allow health insurance companies to underwrite risks......So HHS, the EEOC, the Departments of Labor and Treasury, and the courts have all said our health insurers should be free to assign risk in the same manner car and life insurers do.
Yet the health insurers, for whatever reason, still seem to think they can't.
What Mr. Balko doesn't point out is that under the current system the individual is insulated from their health care costs. To provide the proper incentive such a system of "medical underwriting" would have to exist in a MSA-type program where the individual bore a realistic share of the cost. Another strike against it is the increased prevalence of obesity in individuals with lower socio-economic status could label such a plan as "economic discrimination".
In a nutshell from Mr. Balko's blog TheAgitator
Whodda' thunk that twenty or ten or even five years ago that a major news magazine could pose a question like "are you responsible for your own weight" and not only would there be actual debate on the question, but the "no" side would start the debate with the upper hand?
It's crazy. If you aren't responsible for what you put into your mouth, chew and swallow, what's left that you are you responsible for?
What indeed? |
Apparently one of Dr. Parker's favorite tourist spots has played host to a nanny-state conference on obesity the past few days. Radley Balko has been covering it in TechCentralStation posts here, here, and here. As well as at the Cato Institute and his own blog. From what the Surgeon-General has to say, Mr. McBride should be very afraid:
If you check out the website for the Obesity Summit, you'll notice on the homepage the quote the summit's organizers have chosen to set the tone for three day event. It's from U.S. Surgeon General Richard Carmona:
"As we look to the future and where childhood obesity will be in 20 years... it is every bit as threatening to us as is the terrorist threat we face today. It is the threat from within."
The U.S. government's spokesperson on medical issues says obesity is every bit as threatening as terrorism. Given that the war on terror has spawned the largest federal bureaucracy in the history of the country, questionable trespasses on our civil liberties, and is costing U.S. taxpayers tens of billions of dollars, that's an awfully scary thing for a high-ranking government official to say. And that conference organizers chose to place Carmona's quote front and center ought to give some sort of indication of the starting point from which this debate's about to kick off."
So I guess that means the deck is stacked already. The third TCS article is an excellent analysis of the myth that medical underwriting is illegal:
When I was originally asked to write the designated dissent piece for TIME's special issue on obesity, I went back and forth with a fact-checker over my assertion that state and federal governments prevented health insurers from tying health insurance premiums to risk -- the same way car and life insurers do. Charging everyone within a group plan the same amount for health insurance removes an important financial incentive to stay healthy, and forces fit people to subsidize health care for the not-so-fit. Allowing folks who keep the weight off and the blood pressure and cholesterol down to pay less for health insurance (and allowing health insurers to provide it to them) would also strike a needed blow for personal responsibility in the obesity debate.
The problem is that though several health care policy experts told me they were certain health insurers were barred from such "medical underwriting," no one could say exactly why. In fact, I talked to several health insurance companies themselves, and none could point to any specific law, regulation, or case law laying out the prohibition. I even called tort king John Banzhaf, who -- believe it or not -- is actually on record supporting lower premiums for fit health care consumes, though only as it applies to obesity and blood pressure.....I called the general counsel's office at HHS. Deputy General Counsel Paula Stannard walked me through every possible federal barrier to medical underwriting, and explained why they don't apply.
In fact, in 2001 the Depts. of HHS, Labor and the Treasury (in predictable federal bureaucratic confusion, the three agencies share jurisdiction over the issue) proposed a regulation (66 Fed. Reg. 1421) insisting that the convoluted HIPAA (Health Insurance Portability and Accountability Act) regulations be interpreted to allow health insurance companies to underwrite risks......So HHS, the EEOC, the Departments of Labor and Treasury, and the courts have all said our health insurers should be free to assign risk in the same manner car and life insurers do.
Yet the health insurers, for whatever reason, still seem to think they can't.
What Mr. Balko doesn't point out is that under the current system the individual is insulated from their health care costs. To provide the proper incentive such a system of "medical underwriting" would have to exist in a MSA-type program where the individual bore a realistic share of the cost. Another strike against it is the increased prevalence of obesity in individuals with lower socio-economic status could label such a plan as "economic discrimination".
In a nutshell from Mr. Balko's blog TheAgitator
Whodda' thunk that twenty or ten or even five years ago that a major news magazine could pose a question like "are you responsible for your own weight" and not only would there be actual debate on the question, but the "no" side would start the debate with the upper hand?
It's crazy. If you aren't responsible for what you put into your mouth, chew and swallow, what's left that you are you responsible for?
What indeed? |
Friday, June 04, 2004
SUPPORT YOUR LOCAL MEDICAL ASSOCIATION:
Dr. Smith had an interesting post yesterday in which she answered a reader's email about the lack of unity in medicine. I wanted to comment on this question and answer:
3. Who should lead & speak for doctors in Ohio?
That's a tough one. I guess the Ohio State Medical Association should, but not every doctor is a member. Professional organizations, like the American Medical Association and its sister organizations in each state, are widely perceived as being too narrowly focused on the needs of sub-interests within the organization. Primary care doctors think they cater to the needs of specialists over primary care, and vice versa. Which makes it difficult to unite all of us, contributing to the problems noted in questions one and two
My experience at the county medical society level is that the difference is mainly generational rather than one of specialty. Most of the physicians who attend my local medical society meetings are older, and the younger ones are usually the children of physicians who have been going for years. The younger physicians when asked about their lack of enthusiasm reply with a variety of reasons, lack of time to attend meetings and a desire to spend time with family being the main ones. This inevitably leads to a rant from the older physicians about how they never took time to go see ballgames, or plays, or recitals. While not overt, there sometimes is an veiled questioning of the younger physician's professionalism or dedication.
My personal opinion is that I have better things to do with my time than go to the meetings. See more on my October 14, 2003 post. |
Dr. Smith had an interesting post yesterday in which she answered a reader's email about the lack of unity in medicine. I wanted to comment on this question and answer:
3. Who should lead & speak for doctors in Ohio?
That's a tough one. I guess the Ohio State Medical Association should, but not every doctor is a member. Professional organizations, like the American Medical Association and its sister organizations in each state, are widely perceived as being too narrowly focused on the needs of sub-interests within the organization. Primary care doctors think they cater to the needs of specialists over primary care, and vice versa. Which makes it difficult to unite all of us, contributing to the problems noted in questions one and two
My experience at the county medical society level is that the difference is mainly generational rather than one of specialty. Most of the physicians who attend my local medical society meetings are older, and the younger ones are usually the children of physicians who have been going for years. The younger physicians when asked about their lack of enthusiasm reply with a variety of reasons, lack of time to attend meetings and a desire to spend time with family being the main ones. This inevitably leads to a rant from the older physicians about how they never took time to go see ballgames, or plays, or recitals. While not overt, there sometimes is an veiled questioning of the younger physician's professionalism or dedication.
My personal opinion is that I have better things to do with my time than go to the meetings. See more on my October 14, 2003 post. |
![]()





